Germ Cell Tumours: Difference between revisions
Jump to navigation
Jump to search
Urology4all (talk | contribs) |
Urology4all (talk | contribs) |
||
| (96 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Background == | == Background == | ||
* ''' | * '''Testicular tumours are classified as Germ Cell Tumours (GCTs) vs. non-GCTs''' | ||
**'''95% of testicular tumours are GCTs''' | |||
** 5% of testicular tumours are [[Non-Germ Cell Tumours & Tumours of the Testicular Adnexa|non-germ cell tumours]] such as sex-cord stromal tumours, adenocarcinoma of the rete testis, and lymphoma | ** 5% of testicular tumours are [[Non-Germ Cell Tumours & Tumours of the Testicular Adnexa|non-germ cell tumours]] such as sex-cord stromal tumours, adenocarcinoma of the rete testis, and lymphoma | ||
* '''95% of GCTs originate in the testicle''' | * '''95% of GCTs originate in the testicle''' | ||
** '''5% of GCTs originate outside the testicle i.e. primary extra-gonadal GCT''' | ** '''5% of GCTs originate outside the testicle i.e. primary extra-gonadal GCT''' (see below) | ||
== Epidemiology == | == Epidemiology == | ||
| Line 10: | Line 11: | ||
=== Incidence === | === Incidence === | ||
* '''Relatively rare''' | * '''Relatively rare''' | ||
* Estimated incidence | * Estimated annual incidence | ||
** Worldwide 2020: 74,458 (compared to 1,414,259 for prostate)[https://pubmed.ncbi.nlm.nih.gov/33538338/] | ** Worldwide 2020: 74,458 (compared to 1,414,259 for prostate)[https://pubmed.ncbi.nlm.nih.gov/33538338/] | ||
** US 2021: 9,470[https://seer.cancer.gov/statfacts/html/testis.html] | ** US 2021: 9,470[https://seer.cancer.gov/statfacts/html/testis.html] | ||
*** '''Accounts for 1-2% of cancers among males in the United States''' | *** '''Accounts for 1-2% of cancers among males in the United States''' | ||
* '''Age''' | * '''Age''' | ||
** '''Most common malignancy among males aged 20- | ** '''Most common malignancy among males aged 20-39 years old[https://seer.cancer.gov/statistics-network/explorer/application.html]''' | ||
=== Mortality === | === Mortality === | ||
* Worldwide 2020: 9,334[https://pubmed.ncbi.nlm.nih.gov/33538338/] | * Estimated annual mortality | ||
* US 2021: 440[https://seer.cancer.gov/statfacts/html/testis.html] | **Worldwide 2020: 9,334[https://pubmed.ncbi.nlm.nih.gov/33538338/] | ||
* 5-year relative survival: 94.9% (compared to prostate 97.5%, bladder 77.1%, and kidney/renal pelvis 75.6%)[https://seer.cancer.gov/statfacts/html/testis.html] | ** US 2021: 440[https://seer.cancer.gov/statfacts/html/testis.html] | ||
== Risk | *** 5-year relative survival: 94.9% (compared to prostate 97.5%, bladder 77.1%, and kidney/renal pelvis 75.6%)[https://seer.cancer.gov/statfacts/html/testis.html] | ||
== Risk Factors == | |||
* '''<span style="color:#ff0000"> | * '''<span style="color:#ff0000">Inherited (3):</span>''' | ||
*# '''<span style="color:#ff0000">Family history of GCT</span>''' | *# '''<span style="color:#ff0000">Family history of GCT</span>''' | ||
*# '''<span style="color:#ff0000">Germ Cell Neoplasia In-Situ (GCNIS)</span>''' | |||
*# '''<span style="color:#ff0000">Germ Cell Neoplasia In-Situ (GCNIS)</span> | *#* Previously referred to as intratubular germ cell neoplasia (ITGCN) unclassified | ||
*#* '''All adult invasive GCTs arise from GCNIS, except spermatocytic seminoma.''' | *#*'''All adult invasive GCTs arise from GCNIS, except spermatocytic seminoma.''' | ||
*#* Among males with GCNIS, the risk of developing invasive GCT is ≈50% at 5 years | *#* Among males with GCNIS, the risk of developing invasive GCT is ≈50% at 5 years | ||
*#* '''GCNIS develops before birth from an arrested gonocyte''' | *#* '''GCNIS develops before birth from an arrested gonocyte''' | ||
*# '''<span style="color:#ff0000">Race</span>''' | *# '''<span style="color:#ff0000">Race</span>''' | ||
*#* '''Caucasian risk > African-American''' | *#* '''Caucasian risk > African-American''' | ||
*'''<span style="color:#ff0000">Acquired (2):</span>''' | |||
*#'''<span style="color:#ff0000">Cryptorchidism</span>''' | |||
*#* '''Ipsilateral testis: relative risk 4-6x; relative risk decreases to 2-3x if orchidopexy is performed before puberty''' | |||
*#* '''Contralateral testis: slightly increased risk''' (relative risk 1.74x) | |||
*#'''<span style="color:#ff0000">Personal history of GCT</span>''' | |||
== Genetics == | == Genetics == | ||
| Line 46: | Line 48: | ||
=== Classification === | === Classification === | ||
* '''<span style="color:#ff0000">Pathological: GCNIS-derived vs. non-GCNIS-derived</span>[https://pubmed.ncbi.nlm.nih.gov/27747907/]''' | * '''<span style="color:#ff0000">Pathological: GCNIS-derived vs. non-GCNIS-derived</span>[https://pubmed.ncbi.nlm.nih.gov/27747907/]''' | ||
* '''<span style="color:#ff0000">Clinical: seminoma vs. NSGCT</span>''' | * '''<span style="color:#ff0000">Clinical: seminoma vs. non-seminoma GCT (NSGCT)</span>''' | ||
** '''<span style="color:#ff0000">GCTs that contain both NSGCT subtypes | ** '''<span style="color:#ff0000">GCTs that contain both seminoma and NSGCT subtypes are classified as NSGCTs</span>''' | ||
** Clinical classification based on differences in management and outcome | ** Clinical classification is based on differences in management and outcome | ||
=== Seminoma === | === Seminoma === | ||
* '''<span style="color:#ff0000">Most common type of GCT</span>''' | * '''<span style="color:#ff0000">Most common type of GCT</span>''' | ||
** '''<span style="color:#ff0000">Comprises 52-56% of all GCTs (NSGCT comprises 44-48%)</span>''' | ** '''<span style="color:#ff0000">Comprises 52-56% of all GCTs (NSGCT comprises 44-48%)</span>''' | ||
* ''' | * '''Occurs at an older average age than NSGCTs''' | ||
* '''Arises from GCNIS and is considered to be the common precursor for the other NSGCT subtypes''' | **Most seminoma cases diagnosed in the 4th-5th decade of life | ||
* '''<span style="color:#ff0000">Arises from GCNIS and is considered to be the common precursor for the other NSGCT subtypes</span>''' | |||
=== Non-seminoma === | === Non-seminoma === | ||
| Line 63: | Line 66: | ||
*# '''<span style="color:#ff0000">Choriocarcinoma</span>''' | *# '''<span style="color:#ff0000">Choriocarcinoma</span>''' | ||
*#* '''Rare''' | *#* '''Rare''' | ||
*#* '''Aggressive | *#* '''Aggressive''' | ||
*#* '''<span style="color:#ff0000">Commonly spreads by hematogenous routes</span>''' | *#*'''<span style="color:#ff0000">Commonly spreads by hematogenous routes</span>''' | ||
*#*'''<span style="color:#ff0000">Typically manifests with extremely highly elevated serum hCG levels</span>''' | |||
*# '''<span style="color:#ff0000">Yolk sac tumour</span>''' | *# '''<span style="color:#ff0000">Yolk sac tumour</span>''' | ||
*#* '''Almost always produce AFP but not hCG''' | *#* '''Almost always produce AFP but not hCG''' | ||
*# '''<span style="color:#ff0000">Teratoma</span>''' | *# '''<span style="color:#ff0000">Teratoma</span>''' | ||
*#* '''<span style="color:#ff0000">Histologically benign tumors | *#* '''<span style="color:#ff0000">Histologically benign tumors</span>''' | ||
*#**Contain well-differentiated or incompletely differentiated elements of at least 2/3 germ cell layers: endoderm, mesoderm, and ectoderm. | |||
*#* '''No clinical significance to the distinction between mature and immature teratomas''', and histopathologists do not typically distinguish between the two entities. | *#* '''No clinical significance to the distinction between mature and immature teratomas''', and histopathologists do not typically distinguish between the two entities. | ||
*#* '''Generally associated with normal serum tumor markers, but may cause mildly elevated AFP''' | *#* '''Generally associated with normal serum tumor markers, but may cause mildly elevated AFP''' | ||
| Line 83: | Line 88: | ||
* '''<span style="color:#ff0000">Rapidly growing tumours</span>''' | * '''<span style="color:#ff0000">Rapidly growing tumours</span>''' | ||
=== Metastasis === | |||
==== <span style="color:#ff0000">Sites of metastasis</span> ==== | |||
* '''<span style="color:#ff0000">Lymph nodes</span>''' | |||
** '''<span style="color:#ff0000">Retroperitoneal lymph nodes</span>''' | |||
*** '''<span style="color:#ff0000">Most common site of metastasis</span>''' | |||
**** '''70-80% of GCT metastasis occurs by lymphatic spread''' from the primary tumor to the retroperitoneal lymph nodes and subsequently to distant sites. | |||
***** '''Exception: choriocarcinoma, with a propensity for hematogenous dissemination.''' | |||
** '''<span style="color:#ff0000">Supraclavicular lymph nodes</span>''' | |||
** '''<span style="color:#ff0000">Mediastinal lymph nodes</span>''' | |||
** '''<span style="color:#ff0000">Inguinal lymph nodes in patients with previous scrotal violation</span>''' | |||
* '''<span style="color:#ff0000">Visceral</span>''' | |||
** '''<span style="color:#ff0000">Lung</span>''' | |||
*** '''<span style="color:#ff0000">Second most common site of metastasis</span>''' | |||
*** '''<span style="color:#ff0000">Most common site of visceral metastases</span>''' | |||
***Pulmonary metastases of testicular GCT represents disease spread via the hematogenous route, whereas mediastinal and cervical metastases represent lymphatic spread. | |||
*** '''Thoracic metastasis in the absence of retroperitoneal disease and/or elevated serum tumor markers is uncommon''' | |||
** '''<span style="color:#ff0000">Liver</span>''' | |||
*'''At the time of diagnosis, metastasis''' (regional or distant) '''is present in 33% of cases of NSGCT and 15% of cases of pure seminoma''' | |||
== Diagnosis and Evaluation == | == Diagnosis and Evaluation == | ||
| Line 105: | Line 113: | ||
*# '''<span style="color:#ff0000">History and Physical exam</span>''' | *# '''<span style="color:#ff0000">History and Physical exam</span>''' | ||
*# '''<span style="color:#ff0000">Labs (1):</span>''' | *# '''<span style="color:#ff0000">Labs (1):</span>''' | ||
*## '''<span style="color:#ff0000">Serum tumour markers</span>''' | *## '''<span style="color:#ff0000">Serum tumour markers (AFP, hCG, LDH)</span>''' | ||
*# '''<span style="color:#ff0000">Imaging</span>''' | *# '''<span style="color:#ff0000">Imaging</span>''' | ||
*#* '''<span style="color:#ff0000">Primary: scrotal US with doppler</span>''' | *#* '''<span style="color:#ff0000">Primary: scrotal US with doppler</span>''' | ||
| Line 111: | Line 119: | ||
*#** '''<span style="color:#ff0000">Regional: CT abdomen/pelvis</span>''' | *#** '''<span style="color:#ff0000">Regional: CT abdomen/pelvis</span>''' | ||
*#** '''<span style="color:#ff0000">Distant: CT chest</span>''' (CXR can be used instead of CT if CS I seminoma) | *#** '''<span style="color:#ff0000">Distant: CT chest</span>''' (CXR can be used instead of CT if CS I seminoma) | ||
=== History and Physical Exam === | === History and Physical Exam === | ||
* '''<span style="color:#ff0000"> | ==== History ==== | ||
** '''<span style="color:#ff0000">Most common presentation of testicular cancer: painless | * '''<span style="color:#ff0000">Signs and Symptoms</span>''' | ||
*** '''A firm intratesticular mass should be managed as a malignant neoplasm until proven otherwise and should be evaluated further with a scrotal ultrasound scan.''' | **'''<span style="color:#ff0000">Most common presentation of testicular cancer: painless scrotal mass</span>''' | ||
**'''Symptoms related to metastatic disease (e.g. shortness of breath)''' are the presenting complaint in 10-20% of patients | |||
** | ==== Physical exam ==== | ||
** | * '''Genitourinary''' | ||
** | ** Palpate for any testicular or extra-testicular masses. Note relative size and consistency of affected and normal contralateral testicle. | ||
** | ***'''A firm intratesticular mass should be managed as a malignant neoplasm until proven otherwise and should be evaluated further with a scrotal ultrasound scan.''' | ||
** | ** '''<span style="color:#ff0000">Differential diagnosis of a scrotal mass (8):</span>''' | ||
**# '''<span style="color:#ff0000">Painless</span>''' | |||
** | **##'''<span style="color:#ff0000">Testicular neoplasm</span>''' | ||
** ''' | **##'''<span style="color:#ff0000">Paratesticular neoplasm (benign or malignant)</span>''' | ||
* '''<span style="color:#ff0000"> | **## '''<span style="color:#ff0000">Hernia</span>''' | ||
* | **## '''<span style="color:#ff0000">Varicocele</span>''' | ||
**## '''<span style="color:#ff0000">Spermatocele</span>''' | |||
**#'''<span style="color:#ff0000">Painful</span>''' | |||
** | **##'''<span style="color:#ff0000">Torsion</span>''' | ||
**## '''<span style="color:#ff0000">Hematoma</span>''' | |||
* | **## '''<span style="color:#ff0000">Epididymoorchitis</span>''' | ||
* '''Sites of metastases''' | |||
** | ** '''Supraclavicular lymph nodes''' | ||
** Inguinal lymph nodes, if prior inguinal or scrotal surgery | |||
* '''Gynecomastia''' | |||
** '''Occurs in 2% of males with GCT''' | |||
** Results from elevated serum hCG levels, decreased androgen production, and/or increased estrogen levels | |||
=== Labs === | === Labs === | ||
==== <span style="color:#ff0000">Tumour markers </span><span style="color:#0000ff">(A YET, B SEC)</span> ==== | |||
===== <span style="color:#0000ff">A</span><span style="color:#ff0000">FP</span> ===== | |||
* At diagnosis, elevated in 50-70% of low-stage (CS I, IIA, and IIB) NSGCT and 60-80% of advanced (CS IIC and III) NSGCT | |||
* '''<span style="color:#ff0000">Produced by (3):</span>''' | |||
*# '''<span style="color:#0000ff">Y</span><span style="color:#ff0000">olk sac</span>''' | |||
*# '''<span style="color:#0000ff">E</span><span style="color:#ff0000">C</span>''' | |||
*# '''<span style="color:#0000ff">T</span><span style="color:#ff0000">eratoma</span>''' | |||
** '''<span style="color:#ff0000">Choriocarcinomas and seminomas do not produce AFP</span>''' | |||
*** '''<span style="color:#ff0000">Clinical implication: pure seminoma in the primary tumor with an elevated serum AFP should be treated as NSGCT</span>''' | |||
* '''Upper limit < 11 ng/mL''' | |||
** Despite most laboratories considering AFP > 8ng/mL to be abnormally elevated, a proportion of the population may have levels up to 15-25 ng/mL in the absence of any pathology; '''treatment decisions based solely on “elevated” AFP levels that are stable and <25 ng/mL is discouraged''' | |||
* '''<span style="color:#ff0000">Serum half-life: 5-7 days</span>''' | |||
* '''Other causes of elevated AFP:''' | |||
*# '''Non-malignant liver disease (infectious, drug-induced, alcohol-induced, autoimmune)''' | |||
*# '''Hepatocellular carcinoma''' | |||
*# Cancers of the stomach, pancreas, biliary tract, and lung | |||
*# Ataxic telangiectasia | |||
*# Hereditary tyrosinemia | |||
*# Hereditary persistence of AFP (a congenital alteration in the hepatic nuclear factor binding site of the AFP gene) | |||
===== <span style="color:#0000ff">β</span>-hCG ===== | |||
* At diagnosis, elevated in 20-40% of low-stage NSGCT and 40-60% of advanced NSGCT | |||
* '''<span style="color:#ff0000">Produced by (3):</span>''' | |||
*# '''<span style="color:#0000ff">S</span><span style="color:#ff0000">eminoma (15% of cases)</span>''' | |||
*# '''<span style="color:#0000ff">E</span><span style="color:#ff0000">C</span>''' | |||
*# '''<span style="color:#0000ff">C</span><span style="color:#ff0000">horiocarcinoma</span>''' | |||
* '''Upper limit: <5 mU/mL''' | |||
**'''<span style="color:#ff0000">Levels > 10,000 IU/L are usually associated with choriocarcinoma.</span>''' | |||
* '''<span style="color:#ff0000">Serum half-life: 24 to 36 hours</span>''' (2019 AUA Update Peds Testis Tumours says 24-48 hours) | |||
* '''<span style="color:#ff0000">Other causes of elevated hCG:</span>''' | |||
*# '''<span style="color:#ff0000">Hypogonadism</span>''' | |||
*#* '''<span style="color:#ff0000">LH will be elevated and can be a cause false-positive elevated hCC due to cross-reactivity of the hCG assay with LH</span>''' | |||
*#** '''<span style="color:#ff0000">Supplemental testosterone decreases LH levels, allowing accurate assessment of hCG levels thereafter[https://pubmed.ncbi.nlm.nih.gov/88528/]</span>''' | |||
*# '''Cancers of the liver, biliary tract, pancreas, stomach, lung, breast, kidney, and bladder.''' | |||
*#* The α subunit of hCG is common to several pituitary tumors, and so immunoassays for hCG are directed at the β subunit. | |||
*# '''Cannabis use''' | |||
===== <span style="color:#ff0000">LDH</span> ===== | |||
* At diagnosis, elevated in ≈20% of low-stage GCT and 20-60% of advanced GCT | |||
** | * '''Least relevant and clinically applicable of the tumour markers''' | ||
** | ** Non-specific marker | ||
** '''Main use in GCT is in the''' '''prognostic (S stage classification) assessment at diagnosis.''' | |||
*** '''<span style="color:#ff0000">Serum half-life: | ** '''Treatment decisions based solely on LDH elevation in the setting of normal AFP and hCG should be discouraged.''' | ||
* '''Normal value 48-115 IU/liter''' | |||
**Magnitude of LDH elevation correlates with bulk of disease. | |||
* '''<span style="color:#ff0000">Serum half-life: varies[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3818947/]</span>''' | |||
* LDH is expressed in smooth, cardiac, and skeletal muscles and can be elevated from cancerous (kidney, lymphoma, GI, breast) or non-cancerous conditions (heart failure, anemia, HIV) | |||
===== <span style="color:#ff0000">Pre-orchiectomy tumour markers</span> ===== | |||
* | * '''<span style="color:#ff0000">Uses (2):</span>''' | ||
*# '''<span style="color:#ff0000">Support initial diagnosis</span>''' | |||
*#* '''<span style="color:#ff0000">Should not be used to guide decision making about whether or not to perform a radical orchiectomy''' because AFP or hCG levels in the normal range do not rule out GCT. | |||
*# '''<span style="color:#ff0000">Interpret tumor marker levels after orchiectomy.</span>''' | |||
*#* '''Essential to know whether persistently elevated post-orchiectomy tumour markers are declining compared to pre-orchiectomy levels by their respective half-lives or not, or whether they are rising, as this impacts subsequent treatment decisions.''' | |||
* '''Should not be used for clinical staging and risk stratification''' | |||
** Can lead to over- or under-treatment with resulting excess rates of toxicity or relapse, respectively. | |||
===== <span style="color:#ff0000">Post-orchiectomy tumour markers</span> ===== | |||
* '''<span style="color:#ff0000">Uses (2):</span>''' | |||
*# '''<span style="color:#ff0000">Evaluate for metastases in the case of persistently elevated/rising post-orchiectomy tumour markers</span>''' | |||
*#* Tumour marker levels should normalize after 4 half-lives[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3818947] | |||
*#**Serum AFP levels should return to normal levels 20–28 days after effective therapy. | |||
*#*If borderline elevated (within 3x upper limit of normal) post-orchiectomy markers (AFP and hCG), confirm a rising trend before management decisions are made as false-positive elevations may occur. | |||
*# '''<span style="color:#ff0000">Evaluate for recurrence during surveillance and after completion of therapy (chemotherapy, radiation, surgery).</span>''' | |||
=== Imaging === | === Imaging === | ||
=== Local === | |||
==== Modality ==== | |||
===== Scrotal ultrasound with doppler ===== | |||
* '''<span style="color:#ff0000">Important to evaluate both testicles given</span>''' '''<span style="color:#ff0000">2% incidence of bilateral GCT</span>''' | |||
**'''In cases of bilateral GCT, a metachronous lesion is the most common presentation.''' | |||
* '''High-frequency transducers (5 to 10 MHz)''' can readily identify and distinguish intratesticular lesions a few millimeters in size from extra-testicular pathology | |||
* '''<span style="color:#ff0000">Indications in the context of suspected GCT (3)</span>''' | |||
*# '''<span style="color:#ff0000">Scrotal mass</span>''' | |||
** | *# '''<span style="color:#ff0000">Suspected metastatic GCT with a normal testicular examination</span>''' | ||
*#* '''A small, impalpable scar or calcification indicates a <span style="color:#ff0000">“burned-out” primary testis tumor.</span>''' | |||
*#** '''<span style="color:#ff0000">If sonographic evidence of intratesticular lesions (discrete nodule, stellate scar, coarse calcification), perform radical orchiectomy because GCNIS and residual teratoma are frequently encountered.</span>''' | |||
*# '''<span style="color:#ff0000">Suspected primary extra-gonadal GCT</span>''' | |||
*#* '''<span style="color:#ff0000">Males with advanced GCT with normal testes on physical examination and ultrasound scan are considered to have primary extragonadal GCT.</span>''' | |||
** '''Patients with normal serum tumor markers (hCG and AFP) and indeterminate findings on physical exam or testicular ultrasound for testicular neoplasm should undergo repeat imaging in 6-8 weeks.''' | |||
* '''Imaging findings''' | |||
** '''Typical GCT is hypoechoic''' | |||
** 2 or more discrete lesions may be identified | |||
** INSERT IMAGE | |||
** '''<span style="color:#ff0000">Testicular microlithiasis</span>''' | |||
*** '''Unclear significance''' '''in the general population''' | |||
**** If no history of GCT, risk of GCT is only increased if an additional established risk factor (see above) is present | |||
**** If history of GCT, microlithiasis on ultrasound of the contralateral testis is associated with an increased risk of ITGCN. | |||
*** '''<span style="color:#ff0000">Management</span>''' | |||
**** '''<span style="color:#ff0000">No further evaluation or screening in incidentally detected microlithiasis</span>''' | |||
**** '''<span style="color:#ff0000">If established risk factor and testicular microlithiasis, counsel patient about the potential increased risk of GCT, need for periodic self-examination and follow-up with a medical professional</span>''' | |||
*** insert image | |||
* | ===== MRI ===== | ||
* '''<span style="color:#ff0000">Can be considered an adjunct to scrotal ultrasound in patients with lesions suspicious for benign etiology</span>''' | |||
* '''Should not delay orchiectomy in patients in whom malignancy is suspected''' | |||
=== Metastasis === | |||
==== Regional ==== | |||
* Regional lymph nodes comprises (7): | |||
*# Inter-aortocaval | |||
*# Para-aortic | |||
*# Para-caval | |||
*# Pre-aortic | |||
*# Pre-caval | |||
*# Retro-aortic | |||
*# Retro-caval | |||
* '''<span style="color:#ff0000">Modality</span>''' | |||
** '''<span style="color:#ff0000">CT abdomen/pelvis with oral and IV contrast</span>''' | |||
**** | *** '''<span style="color:#ff0000">Most effective imaging modality for regional staging</span>''' | ||
** MRI | |||
*** | *** Alternative to CT | ||
* '''<span style="color:#ff0000">Imaging findings</span>''' | |||
** '''<span style="color:#ff0000">Retroperitoneal lymph nodes</span>''' | |||
** | *** '''<span style="color:#ff0000">Pattern of lymph drainage in the retroperitoneum is from right to left.</span>''' | ||
*** | **** '''<span style="color:#ff0000">For right testis tumors, the primary drainage site is the inter-aortocaval lymph nodes inferior to the renal vessels, followed by the paracaval and para-aortic nodes.</span>''' | ||
**** '''<span style="color:#ff0000">For left testis tumors, the primary drainage site is the para-aortic lymph nodes, followed by the inter-aortocaval nodes.</span>''' | |||
*** | *** [[File:Retroperitoneal lymph flow.jpg|thumb|Direction of lymphatic flow in the retroperitoneum]] | ||
** '''<span style="color:#ff0000">"Borderline" retroperitoneal lymph nodes</span>''' | |||
*** '''<span style="color:#ff0000">Lymph nodes 5-9 mm in the primary landing zone should be viewed with suspicion for regional lymph node metastasis,</span> particularly if they are anterior to the great vessels''' | |||
** '''Limitations''' | |||
*** '''Understaging''' | |||
**** 25-35% of patients with CSI NSGCT and a “normal” CT scan will be found to have pathologically involved retroperitoneal lymph nodes at RPLND | |||
*** '''Overstaging''' | |||
**** 12-40% of patients with CS IIA and IIB disease will be found to have pathologically negative lymph nodes at RPLND | |||
==== Distant ==== | |||
* '''<span style="color:#ff0000">Chest</span>''' | |||
** '''<span style="color:#ff0000">Timing</span>''' | |||
*** '''<span style="color:#ff0000">Necessary to complete staging in patients with confirmed GCTs</span>''' | |||
*** '''<span style="color:#ff0000">Should not delay orchiectomy</span>''' | |||
** '''<span style="color:#ff0000">Modality: plain-film chest x-ray vs. CT</span>''' | |||
*** '''<span style="color:#ff0000">Chest x-ray</span>''' | |||
**** '''<span style="color:#ff0000">Indications</span>[https://pubmed.ncbi.nlm.nih.gov/31059667/ ★]''' | |||
**** | ***** '''<span style="color:#ff0000">Suspected clinical stage I seminoma</span>'''; preferred over CT | ||
****** '''When tumor markers are normal, the rate of skip metastasis to the thorax in seminoma is close to 0%,''' and the addition of CT chest to chest x-ray is very unlikely to alter treatment decisions. | |||
**** '''No role for routine bone scintigraphy or brain CT imaging at the time of diagnosis.''' | *** '''<span style="color:#ff0000">CT scan</span>''' | ||
**** | **** '''<span style="color:#ff0000">Indications (3)</span>[https://pubmed.ncbi.nlm.nih.gov/31059667/ ★]''' | ||
****# '''<span style="color:#ff0000">NSGCT</span>''' | |||
****#* '''Skip metastases are more common in non-seminoma than seminoma.''' | |||
****# '''<span style="color:#ff0000">Elevated and rising post-orchiectomy markers (hCG and AFP)</span>''' | |||
****# '''<span style="color:#ff0000">Any evidence of metastases on abdominal/pelvic imaging, chest x-ray or physical exam.</span>''' | |||
* '''Other''' | |||
** '''Bone scan and CT brain''' | |||
***'''No role for routine bone scintigraphy or brain CT imaging at the time of diagnosis.[https://pubmed.ncbi.nlm.nih.gov/31059667/ ★]''' | |||
**** In the absence of symptoms or other clinical indicators of disease, visceral metastasis to bone and brain is uncommon in GCT | |||
**** '''Indications for bone scan and CT brain (3):''' | |||
****#'''Symptoms suggestive of central nervous system or bone involvement''' | |||
****# '''Poor prognosis disease.''' | |||
****#'''Highly elevated hCG (>10,000 mU/mL)''' | |||
****#*'''<span style="color:#ff0000">Highly elevated hCG are often associated with metastatic choriocarcinoma, which has a propensity for brain metastases.</span>''' | |||
** '''<span style="color:#ff0000">FDG-PET</span>''' | |||
*** '''<span style="color:#ff0000">Currently, no role in the routine evaluation of NSGCT and seminoma at the time of diagnosis.</span>''' | |||
=== Other === | === Other === | ||
* '''Testicular biopsy: contraindicated''' | * '''<span style="color:#ff0000">Testicular biopsy: contraindicated</span>''' | ||
** '''Scrotal violation increases risk of (2):''' | ** '''Scrotal violation increases risk of (2):''' | ||
**# '''Pelvic or inguinal lymph node metastasis due to altered lymphatic drainage of the testicle''' | **# '''Pelvic or inguinal lymph node metastasis due to altered lymphatic drainage of the testicle''' | ||
**# '''Local recurrence''' | **# '''Local recurrence''' | ||
*** '''Systematic review of outcomes of scrotal violation in testicular cancer''' | *** '''<span style="color:#ff00ff">Systematic review of outcomes of scrotal violation in testicular cancer</span>''' | ||
**** Scrotal violation defined at non-standard surgical approaches including trans-scrotal orchiectomy, open testicular biopsy, and fine needle aspiration | **** Scrotal violation defined at non-standard surgical approaches including trans-scrotal orchiectomy, open testicular biopsy, and fine needle aspiration | ||
**** '''Results''' | **** '''Results''' | ||
| Line 296: | Line 324: | ||
***** Among patients undergoing excision of the scrotal scar, 9% had residual, viable GCT. | ***** Among patients undergoing excision of the scrotal scar, 9% had residual, viable GCT. | ||
***** '''No difference in rates of metastatic disease or all-cause mortality based on scrotal violation''' | ***** '''No difference in rates of metastatic disease or all-cause mortality based on scrotal violation''' | ||
**** Capelouto, Carl C., et al."Testis cancer: a review of scrotal violation in testicular cancer: is adjuvant local therapy necessary?." ''The Journal of urology'' 153.3 (1995): 981-985. | **** Capelouto, Carl C., et al."[https://pubmed.ncbi.nlm.nih.gov/7853587/ Testis cancer: a review of scrotal violation in testicular cancer: is adjuvant local therapy necessary?.]" ''The Journal of urology'' 153.3 (1995): 981-985. | ||
== Staging == | == Staging == | ||
=== TNM (AJCC 8th edition§) === | |||
==== T stage (primary tumor) ==== | |||
* '''pTX''': cannot be assessed | |||
* '''pT0''': no evidence of primary tumour | |||
* '''pTis''': germ cell neoplasia in situ | |||
* '''<span style="color:#ff0000">pT1: tumour limited to testis (including rete testis invastion) without lymphovascular invasion (LVI)</span>''' | |||
** '''<span style="color:#ff0000">For pure seminoma:</span>''' | |||
*** '''<span style="color:#ff0000">pT1a: tumour size < 3 cm</span>''' | |||
*** '''<span style="color:#ff0000">pT1b: tumour size ≥ 3 cm</span>''' | |||
* '''<span style="color:#ff0000">pT2: tumour limited to testis (including rete testis invastion) with LVI or tumour invading hilar soft tissue, epididymis or tunica vaginalis</span>''' | |||
* '''<span style="color:#ff0000">pT3: direct (continuous) spermatic cord soft tissue invasion</span>''' | |||
** LVI of the spermatic cord without soft tissue invasion is not pT3 | |||
* '''<span style="color:#ff0000">pT4: direct scrotum invasion</span>''' | |||
==== N Stage (regional lymph node stage) ==== | |||
* '''<span style="color:#ff0000">Clinical</span>''' | |||
** cNX: regional lymph nodes cannot be assessed | |||
** cN0: no regional lymph node metastasis | |||
** '''<span style="color:#ff0000">cN1: metastasis with a lymph node mass <u>≤2 cm</u> in greatest dimension OR multiple lymph nodes, each <u>≤2 cm</u> cm in greatest dimension</span>''' | |||
** '''<span style="color:#ff0000">cN2: metastasis with a lymph node mass <u>>2 cm but ≤5</u> cm in greatest dimension OR multiple lymph nodes, any one mass >2 cm but ≤5 cm</span>''' | |||
** '''<span style="color:#ff0000">cN3: metastasis with a lymph node mass <u>>5 cm</u> in greatest dimension'''</span> | |||
* '''Pathologic''' | |||
** pNX''':''' regional lymph nodes cannot be assessed | |||
** pN0: no regional lymph node metastasis | |||
** '''pN1:''' metastasis with a lymph node mass '''≤2 cm''' in greatest dimension '''AND ≤5 positive nodes''', none >2 cm in greatest dimension | |||
** '''pN2:''' | |||
*** Metastasis with a lymph node mass '''>2 cm but ≤5 cm''' in greatest dimension '''OR''' | |||
*** '''>5 nodes positive,''' none >5 cm in greatest dimension OR | |||
*** '''Extranodal extension of tumour''' | |||
** pN3: metastasis with a lymph node mass '''>5 cm''' in greatest dimension | |||
==== M stage (distant metastasis) ==== | |||
* MX: distant metastasis cannot be assessed | |||
* M0: no distant metastasis | |||
* '''M1a: non-regional lymph node (ex: iliac, inguinal, pelvic NOS) or lung metastasis''' | |||
* '''M1b: non-lung visceral metastasis''' | |||
==== S stage (serum markers) ==== | |||
* '''SX''': serum tumor markers not available or not performed | |||
* '''S0''': markers within normal limits | |||
* '''S1: LDH < 1.5 x upper limit of normal, hCG < 5,000 mIU/mL and AFP < 1,000 ng/mL''' | |||
* '''S2: LDH 1.5 - 10 x upper limit of normal OR hCG 5,000 - 50,000 mIU/mL OR AFP 1,000 - 10,000 ng/mL''' | |||
* '''S3: LDH > 10 x upper limit of normal OR hCG > 50,000 mIU/mL OR AFP > 10,000 ng/mL''' | |||
=== Clinical staging === | |||
* '''<span style="color:#ff0000">Prognosis of GCT and initial management decisions are determined by clinical stage (CS)''' | |||
* '''<span style="color:#ff0000">Based on (3):''' | |||
*# '''<span style="color:#ff0000">Pathologic stage of the primary tumour (pT stage)''' | |||
*# '''<span style="color:#ff0000">Presence and extent of regional (N stage) and distant metastatic disease (M stage)''' | |||
*# '''<span style="color:#ff0000">Post-orchiectomy serum tumor marker levels (S stage)''' | |||
*#* Serum tumor markers (AFP, hCG, and LDH) should be repeated at appropriate T1/2 time intervals after orchiectomy to determine nadir for staging and risk stratification | |||
*#** For patients with elevated AFP or hCG post-orchiectomy, clinicians should monitor serum tumor markers to establish nadir levels before treatment only if marker nadir levels would influence treatment. | |||
* '''Testicular cancer clinical stage groups''' | |||
{| class="wikitable" | {| class="wikitable" | ||
| Line 471: | Line 504: | ||
|} | |} | ||
* '''Overview of clinical staging:''' | * '''<span style="color:#ff0000">Overview of clinical staging:</span>''' | ||
** '''Clinical stage (CS) I: disease confined to the testis''' | ** '''<span style="color:#ff0000">Clinical stage (CS) I: disease confined to the testis</span>''' | ||
** '''CS II: presence of regional (retroperitoneal) lymph node metastasis''' | ** '''<span style="color:#ff0000">CS II: presence of regional (retroperitoneal) lymph node metastasis</span>''' | ||
** '''CS III: non-regional lymph node and/or visceral metastasis, although post-orchiectomy serum tumour marker levels can upstage patients from CSII to CSIII''' | ** '''<span style="color:#ff0000">CS III: non-regional lymph node and/or visceral metastasis, although post-orchiectomy serum tumour marker levels can upstage patients from CSII to CSIII</span>''' | ||
== Management == | == Management == | ||
| Line 484: | Line 517: | ||
** '''Review of primary tumor specimens by experienced pathologists is recommended.''' | ** '''Review of primary tumor specimens by experienced pathologists is recommended.''' | ||
*** Expert review of pathologic specimens should be considered in clinical scenarios where treatment decisions will be impacted. | *** Expert review of pathologic specimens should be considered in clinical scenarios where treatment decisions will be impacted. | ||
**** | **** Studies have shown that expert pathology review can change the pathological subtype in 1-4% of cases.[https://pubmed.ncbi.nlm.nih.gov/16045777/][https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7704081/] | ||
* '''Management decisions should be based on imaging obtained within the preceding 4 weeks and serum tumor markers (hCG and AFP) within the preceding 10 days.''' | * '''<span style="color:#ff0000">Management decisions should be based on imaging obtained within the preceding 4 weeks and serum tumor markers (hCG and AFP) within the preceding 10 days.</span>''' | ||
** Due to the rapid | ** Due to the rapid growth of many GCT, particularly NSGCT, there is a risk of disease progression between staging studies and intervention. Therefore, risk adapted management decisions (i.e. RPLND for Stage IIA disease) should be made based on recent imaging and serum tumor marker levels to avoid undertreatment. | ||
* '''In patients with normal serum tumor markers (hCG and AFP) and equivocal imaging findings for metastasis, consider repeat imaging in 6-8 weeks to clarify the extent of disease prior to making a treatment recommendation'''. | * '''In patients with normal serum tumor markers (hCG and AFP) and equivocal imaging findings for metastasis, consider repeat imaging in 6-8 weeks to clarify the extent of disease prior to making a treatment recommendation'''. | ||
* '''Prior to definitive management, patients should be counseled about the risks of (3):''' | * '''<span style="color:#ff0000">Prior to definitive management, patients should be counseled about the risks of (3):</span>''' | ||
*# '''Hypogonadism''' | *# '''<span style="color:#ff0000">Hypogonadism</span>''' | ||
*#* '''Hormone levels in long-term survivors of testicular cancer''' | *#* '''<span style="color:#ff00ff">Hormone levels in long-term survivors of testicular cancer</span>''' | ||
*#** Population: 1235 patients with history of unilateral orchiectomy for testicular cancer and adjuvant RPLND only, radiotherapy only, or chemotherapy | *#** Population: 1235 patients with history of unilateral orchiectomy for testicular cancer and adjuvant RPLND only, radiotherapy only, or chemotherapy | ||
*#** Compared to healthy controls | *#** Compared to healthy controls | ||
| Line 497: | Line 530: | ||
*#*** '''No significant difference in serum testosterone between testicular cancer patients and healthy controls''' | *#*** '''No significant difference in serum testosterone between testicular cancer patients and healthy controls''' | ||
*#*** Significantly higher age-adjusted LH in testicular cancer patients | *#*** Significantly higher age-adjusted LH in testicular cancer patients | ||
*#** Nord, Carina, et al."Gonadal hormones in long-term survivors 10 years after treatment for unilateral testicular cancer." ''European urology'' 44.3 (2003): 322-328. | *#** Nord, Carina, et al. "[https://pubmed.ncbi.nlm.nih.gov/12932930/ Gonadal hormones in long-term survivors 10 years after treatment for unilateral testicular cancer.]" ''European urology'' 44.3 (2003): 322-328. | ||
*#* Over long-term follow-up, up to 10-15% of patients will have low serum testosterone levels or will require testosterone replacement therapy | *#* Over long-term follow-up, up to 10-15% of patients will have low serum testosterone levels or will require testosterone replacement therapy | ||
*# '''Infertility''' | *# '''<span style="color:#ff0000">Infertility</span>''' | ||
*#* '''At diagnosis, up to 50% have impaired semen parameters and 10% are azoospermic''' | *#* '''At diagnosis, up to 50% have impaired semen parameters and 10% are azoospermic''' | ||
*#* '''Sperm cryopreservation''' | *#* '''<span style="color:#ff0000">Sperm cryopreservation</span>''' | ||
*#** '''Timing''' | *#** '''<span style="color:#ff0000">Timing</span>''' | ||
*#*** '''Pre-orchiectomy''' | *#*** '''<span style="color:#ff0000">Pre-orchiectomy</span>''' | ||
*#**** '''Consider in patients without a normal contralateral testicle or with known subfertility''' | *#**** '''Consider in patients without a normal contralateral testicle or with known subfertility''' | ||
*#*** '''Post-orchiectomy''' | *#*** '''<span style="color:#ff0000">Post-orchiectomy</span>''' | ||
*#**** '''Recommended before treatment (other than orchiectomy) is initiated in patients who are undecided or are planning future paternity.''' | *#**** '''Recommended before treatment (other than orchiectomy) is initiated in patients who are undecided or are planning future paternity.''' | ||
*#***** '''Virtually all patients become azoospermic after chemotherapy, and 50-80% of patients with normal semen parameters at diagnosis return to these levels within 2 and 5 years, respectively.''' | *#***** '''Virtually all patients become azoospermic after chemotherapy, and 50-80% of patients with normal semen parameters at diagnosis return to these levels within 2 and 5 years, respectively.''' | ||
*#***** '''Recovery of spermatogenesis after radiation therapy for seminoma may take | *#***** '''Recovery of spermatogenesis after radiation therapy for seminoma may take 2-3 years or longer.''' | ||
*#**** '''Consider in patients with a normal contralateral testicle or known fertility, who''' '''are undecided or are planning future paternity''', given the potential risk of pathologic process (testicular cancer, trauma) involving contralateral testicle | *#**** '''Consider in patients that do not require further treatment with a normal contralateral testicle or known fertility, who''' '''are undecided or are planning future paternity''', given the potential risk of pathologic process (testicular cancer, trauma) involving the normal contralateral testicle | ||
*# '''Contralateral tumour''' | *# '''<span style="color:#ff0000">Contralateral tumour</span>''' | ||
*#* '''Patients with a history of GCT or GCNIS should be informed of risks of a second primary tumor while rare is significantly increased in the contralateral testis''' | *#* '''Patients with a history of GCT or GCNIS should be informed of risks of a second primary tumor, while rare, is significantly increased in the contralateral testis''' | ||
=== Orchiectomy === | === Orchiectomy === | ||
| Line 519: | Line 552: | ||
==== Radical inguinal orchiectomy ==== | ==== Radical inguinal orchiectomy ==== | ||
* '''Testicular prosthesis should be discussed prior to orchiectomy.''' | * '''<span style="color:#ff0000">Testicular prosthesis should be discussed prior to orchiectomy.</span>''' | ||
* '''Approach: inguinal''' | * '''<span style="color:#ff0000">Approach: inguinal</span>''' | ||
** '''Trans-scrotal orchiectomy: contraindicated due to risks of scrotal violation (see above)''' | ** '''<span style="color:#ff0000">Trans-scrotal orchiectomy: contraindicated due to risks of scrotal violation (see above)</span>''' | ||
*** '''Patients who have undergone scrotal orchiectomy for malignant neoplasm should be counseled regarding the increased risk of local recurrence and may rarely be considered for adjunctive therapy (excision of scrotal scar or radiotherapy) for local control''' | *** '''Patients who have undergone scrotal orchiectomy for malignant neoplasm should be counseled regarding the increased risk of local recurrence and may rarely be considered for adjunctive therapy (excision of scrotal scar or radiotherapy) for local control''' | ||
**** In patients that have received systemic therapy following scrotal orchiectomy, local relapse is rare and adjuvant therapy is not needed | **** In patients that have received systemic therapy following scrotal orchiectomy, local relapse is rare and adjuvant therapy is not needed | ||
* '''Patients suspected | * '''<span style="color:#ff0000">Patients suspected of having a testicular neoplasm should undergo a radical inguinal orchiectomy with removal of the tumor-bearing testicle and spermatic cord to the level of the internal inguinal ring.</span>''' | ||
** '''In very rare cases where there is a possibility of a benign tumour, excisional biopsy with a frozen section should be performed prior to definitive orchiectomy to allow for the possibility of organ-sparing partial orchiectomy.''' | ** '''In very rare cases where there is a possibility of a benign tumour, excisional biopsy with a frozen section should be performed prior to definitive orchiectomy to allow for the possibility of organ-sparing partial orchiectomy.''' | ||
* '''Timing''' | * '''<span style="color:#ff0000">Timing</span>''' | ||
** '''In general, orchiectomy should be performed prior to any further treatment.''' | ** '''<span style="color:#ff0000">In general, orchiectomy should be performed prior to any further treatment.</span>''' | ||
*** '''Exception: in patients with life-threatening metastatic disease and an unequivocally elevated AFP and/or HCG, orchiectomy should not delay the start of chemotherapy and can be postponed until later in the treatment course''' | *** '''<span style="color:#ff0000">Exception: in patients with life-threatening metastatic disease and an unequivocally elevated AFP and/or HCG, orchiectomy should not delay the start of chemotherapy and can be postponed until later in the treatment course</span>''' | ||
==== Testis-sparing surgery (TSS) | ==== Testis-sparing surgery (TSS)[https://www.auanet.org/guidelines/testicular-cancer-guideline] ==== | ||
* '''Not recommended in patients with a testicular lesion suspicious for malignant neoplasm and a normal contralateral testis; radical inguinal orchiectomy is recommended''' | * '''<span style="color:#ff0000">Not recommended in patients with a testicular lesion suspicious for malignant neoplasm and a normal contralateral testis; radical inguinal orchiectomy is recommended</span>''' | ||
* '''Indications (3)''' | * '''<span style="color:#ff0000">Indications (3)</span>''' | ||
*# '''Patients wishing to preserve gonadal function''' | *# '''<span style="color:#ff0000">Patients wishing to preserve gonadal function</span>''' | ||
*# '''Mass <2cm''' | *# '''<span style="color:#ff0000">Mass <2cm</span>''' | ||
*# '''And one of the following:''' | *# '''<span style="color:#ff0000">And one of the following:</span>''' | ||
*## '''Equivocal ultrasound/physical exam findings and negative tumor markers (hCG and AFP)''' | *## '''<span style="color:#ff0000">Equivocal ultrasound/physical exam findings and negative tumor markers (hCG and AFP)</span>''' | ||
*## '''Congenital, acquired or functionally solitary testis''' | *## '''<span style="color:#ff0000">Congenital, acquired or functionally solitary testis</span>''' | ||
*## '''Bilateral synchronous tumors''' | *## '''<span style="color:#ff0000">Bilateral synchronous tumors</span>''' | ||
* '''Patients considering TSS should be counseled regarding (5):''' | * '''Patients considering TSS should be counseled regarding (5):''' | ||
*# '''Higher risk of local recurrence''' | *# '''Higher risk of local recurrence''' | ||
| Line 562: | Line 595: | ||
**** '''Radiation''' | **** '''Radiation''' | ||
***** '''Advantage''' | ***** '''Advantage''' | ||
****** ''' | ****** '''Reduced risk of hypogonadism compared to orchiectomy''' | ||
******* '''Leydig cells are | ******* '''Leydig cells are radioresistant compared with germinal epithelium.''' | ||
******* Leydig cell function may decline over time, and 40% of men who receive radiation therapy require supplemental testosterone | ******* Leydig cell function may decline over time, and 40% of men who receive radiation therapy require supplemental testosterone | ||
***** '''Disadvantage''' | ***** '''Disadvantage''' | ||
****** ''' | ****** '''Increased risk of infertility compared to orchiectomy''' | ||
******* '''For patients with a normal contralateral testis who desire future paternity, radical orchiectomy is preferred because scatter to the contralateral testis from radiotherapy may impair spermatogenesis.''' | ******* '''For patients with a normal contralateral testis who desire future paternity, radical orchiectomy is preferred because scatter to the contralateral testis from radiotherapy may impair spermatogenesis.''' | ||
******* Radiation at these doses causes permanent sterility of the treated testis, but can be delayed in patients who wish to father children. | ******* Radiation at these doses causes permanent sterility of the treated testis, but can be delayed in patients who wish to father children. | ||
| Line 588: | Line 621: | ||
=== Post-orchiectomy management === | === Post-orchiectomy management === | ||
* '''Based on histology (seminoma vs. NSGCT) and clinical stage''' | * '''<span style="color:#ff0000">Based on histology (seminoma vs. NSGCT) and clinical stage</span>''' | ||
==== General principles ==== | ==== General principles ==== | ||
* '''Newly elevated and/or rising serum tumor marker levels after orchiectomy indicate the presence of metastatic disease, and these patients should receive induction chemotherapy.''' | * '''<span style="color:#ff0000">Newly elevated and/or rising serum tumor marker levels after orchiectomy indicate the presence of metastatic disease</span>, and these patients should receive induction chemotherapy.''' | ||
* '''In the setting of a negative metastatic evaluation and slowly declining markers (i.e., not according to half-life), patients should be monitored closely and have levels checked periodically until the levels normalize or begin to rise.''' | * '''In the setting of a negative metastatic evaluation and slowly declining markers (i.e., not according to half-life), patients should be monitored closely and have levels checked periodically until the levels normalize or begin to rise.''' | ||
* '''Surveillance for clinical stage I disease''' | * '''Surveillance for clinical stage I disease''' | ||
| Line 604: | Line 637: | ||
**# Risk of second malignant neoplasms owing to intensive surveillance CT imaging | **# Risk of second malignant neoplasms owing to intensive surveillance CT imaging | ||
**# More intensive therapy required to treat patients at the time of relapse than if they had received treatment at diagnosis | **# More intensive therapy required to treat patients at the time of relapse than if they had received treatment at diagnosis | ||
* '''Radiotherapy''' | * '''<span style="color:#ff0000">Radiotherapy</span>''' | ||
** '''Seminoma are sensitive to radiation therapy''' | ** '''<span style="color:#ff0000">Seminoma are sensitive to radiation therapy</span>''' | ||
** '''Radiation therapy has no role in NSGCT with the exception of treatment for brain metastases.''' | ** '''<span style="color:#ff0000">Radiation therapy has no role in NSGCT with the exception of treatment for brain metastases.</span>''' | ||
* '''Chemotherapy''' | * '''<span style="color:#ff0000">Chemotherapy</span>''' | ||
** '''International Germ Cell Cancer Collaborative Group (IGCCCG) risk classification''' | ** '''<span style="color:#ff0000">International Germ Cell Cancer Collaborative Group (IGCCCG) risk classification</span>''' | ||
*** '''Used''' over the TNM system '''to select the chemotherapy regimen and number of cycles in patients receiving chemotherapy for advanced disease''' | *** '''<span style="color:#ff0000">Used</span>''' over the TNM system '''<span style="color:#ff0000">to select the chemotherapy regimen and number of cycles in patients receiving chemotherapy for advanced disease</span>''' | ||
**** '''Developed in patients with metastatic GCT at the time of diagnosis and is NOT applicable to patients with relapsed GCT''' | **** '''<span style="color:#ff0000">Developed in patients with metastatic GCT at the time of diagnosis and is NOT applicable to patients with relapsed GCT</span>''' | ||
*** ''' | *** '''<span style="color:#ff0000">Classified into (3): good, intermediate, and poor prognosis</span>''' | ||
***# '''Presence of non-pulmonary visceral metastasis''' | ***'''<span style="color:#ff0000">Classification based on:</span>''' | ||
***# '''Primary mediastinal NSGCT''' | ****'''<span style="color:#ff0000">NSGCT (3):</span>''' | ||
***# '''TMs at the initiation of chemotherapy (not levels measured before orchiectomy)''' | ****# '''<span style="color:#ff0000">Presence of non-pulmonary visceral metastasis</span>''' | ||
*** ''' | ****# '''<span style="color:#ff0000">Primary mediastinal NSGCT</span>''' | ||
***# '''Presence of non-pulmonary visceral metastasis''' | ****# '''<span style="color:#ff0000">TMs at the initiation of chemotherapy (not levels measured before orchiectomy)</span>''' | ||
***#* '''No poor prognosis category''' | **** '''<span style="color:#ff0000">Seminoma (1):</span>''' | ||
****# '''<span style="color:#ff0000">Presence of non-pulmonary visceral metastasis</span>''' | |||
****#* '''<span style="color:#ff0000">No poor prognosis category</span>''' | |||
{| class="wikitable" | {| class="wikitable" | ||
| Line 670: | Line 705: | ||
** Markedly elevated HCG prior to treatment may take longer to normalize or plateau at the end of chemotherapy | ** Markedly elevated HCG prior to treatment may take longer to normalize or plateau at the end of chemotherapy | ||
* '''RPLND''' | * '''RPLND''' | ||
** See [[RPLND]] Chapter Notes | ** See [[Retroperitoneal Lymph Node Dissection|RPLND]] Chapter Notes | ||
==== Seminoma ==== | ==== Seminoma ==== | ||
| Line 676: | Line 711: | ||
===== CSIA and IB Seminoma ===== | ===== CSIA and IB Seminoma ===== | ||
* '''Options (3):''' | * '''<span style="color:#ff0000">Options (3):</span>''' | ||
** '''Preferred (1): surveillance''' | ** '''<span style="color:#ff0000">Preferred (1): surveillance</span>''' | ||
** '''Alternatives (2):''' | ** '''<span style="color:#ff0000">Alternatives (2):</span>''' | ||
**# '''Adjuvant primary radiotherapy (20 Gy to the para-aortic region)''' | **# '''<span style="color:#ff0000">Adjuvant primary radiotherapy (20 Gy to the para-aortic region)</span>''' | ||
**# '''Adjuvant primary chemotherapy with single-agent carboplatin (1 cycle)''' | **# '''<span style="color:#ff0000">Adjuvant primary chemotherapy with single-agent carboplatin (1 cycle)</span>''' | ||
** '''Both 2019 AUA and 2010 CUA guidelines recommend surveillance, adjuvant as an alternative''' | ** '''<span style="color:#ff0000">Both 2019 AUA and 2010 CUA guidelines recommend surveillance, adjuvant as an alternative</span>''' | ||
*** '''If adjuvant treatment is chosen''' | *** '''If adjuvant treatment is chosen''' | ||
**** '''CUA recommends radiotherapy over chemotherapy''' | **** '''CUA recommends radiotherapy over chemotherapy''' | ||
| Line 687: | Line 722: | ||
**** '''SWONTECA recommends radiotherapy only if chemotherapy not suitable''' | **** '''SWONTECA recommends radiotherapy only if chemotherapy not suitable''' | ||
** Long-term survival rates approaching 100% for each approach | ** Long-term survival rates approaching 100% for each approach | ||
** '''Surveillance for clinical stage I seminoma''' | ** '''<span style="color:#ff0000">Surveillance for clinical stage I seminoma</span>''' | ||
*** 80-85% of patients with clinical stage I seminoma achieve cure with radical orchiectomy alone | *** 80-85% of patients with clinical stage I seminoma achieve cure with radical orchiectomy alone | ||
*** Protocol varies by institution, no consensus | *** Protocol varies by institution, no consensus | ||
| Line 694: | Line 729: | ||
**** Imaging of the chest and serum tumor marker assessment can be obtained as clinically indicated. | **** Imaging of the chest and serum tumor marker assessment can be obtained as clinically indicated. | ||
***** Compared with NSGCT, surveillance for CS I seminoma is complicated by the limited utility of serum tumor markers to detect relapse | ***** Compared with NSGCT, surveillance for CS I seminoma is complicated by the limited utility of serum tumor markers to detect relapse | ||
*** '''Risk factors for relapse on surveillance (2):''' | *** '''<span style="color:#ff0000">Risk factors for relapse on surveillance (2):</span>''' | ||
**** '''Tumor size >4 cm''' | **** '''<span style="color:#ff0000">Tumor size >4 cm</span>''' | ||
**** '''Rete testis invasion''' | **** '''<span style="color:#ff0000">Rete testis invasion</span>''' | ||
*** Patients who relapse on surveillance should be fully restaged and treated based on their TNM-s status. | *** Patients who relapse on surveillance should be fully restaged and treated based on their TNM-s status. | ||
** '''Adjuvant primary radiotherapy''' | ** '''Adjuvant primary radiotherapy''' | ||
| Line 714: | Line 749: | ||
****** Requires serial follow-up CT imaging after treatment | ****** Requires serial follow-up CT imaging after treatment | ||
**** Dog-leg vs. para-aortic | **** Dog-leg vs. para-aortic | ||
***** RTC found para-aortic to be non-inferior to dog-leg radiotherapy in CSI | ***** RTC found para-aortic to be non-inferior to dog-leg radiotherapy in CSI seminoma[https://pubmed.ncbi.nlm.nih.gov/21212385/ §] | ||
** '''Adjuvant primary chemotherapy''' | ** '''Adjuvant primary chemotherapy''' | ||
*** Cisplatin is inferior to carboplatin for CSI seminoma | *** Cisplatin is inferior to carboplatin for CSI seminoma | ||
| Line 722: | Line 757: | ||
* ≈15-20% of patients with seminoma have CS II disease at diagnosis; 70% of these patients have CS IIA and IIB. | * ≈15-20% of patients with seminoma have CS II disease at diagnosis; 70% of these patients have CS IIA and IIB. | ||
* '''CSIIA:''' | * '''<span style="color:#ff0000">CSIIA:</span>''' | ||
** '''CUA: Dog-leg radiotherapy (25-35 Gy) preferred over first-line chemotherapy (BEP×3 or EP×4)''' | ** '''CUA: Dog-leg radiotherapy (25-35 Gy) preferred over first-line chemotherapy (BEP×3 or EP×4)''' | ||
** '''AUA: radiotherapy or chemotherapy''' | ** '''AUA: radiotherapy or chemotherapy''' | ||
* '''CSIIB:''' | * '''<span style="color:#ff0000">CSIIB:</span>''' | ||
** '''CUA: depending on bulk of disease and location of lymph nodes, radiation or chemotherapy [good risk chemotherapy BEP×3 or EP×4] can be used.''' | ** '''CUA: depending on bulk of disease and location of lymph nodes, radiation or chemotherapy [good risk chemotherapy BEP×3 or EP×4] can be used.''' | ||
*** '''First-line chemotherapy is recommended for bulky (>3 cm) and/or multifocal retroperitoneal metastases''' | *** '''First-line chemotherapy is recommended for bulky (>3 cm) and/or multifocal retroperitoneal metastases''' | ||
| Line 732: | Line 767: | ||
*** '''CSIIB with lymph node >3cm: chemotherapy''' | *** '''CSIIB with lymph node >3cm: chemotherapy''' | ||
* Routine surveillance CT imaging is unnecessary after complete resolution of disease. | * Routine surveillance CT imaging is unnecessary after complete resolution of disease. | ||
*'''<span style="color:#ff00ff">Surgery in Early Metastatic Seminoma (SEMS) Trial</span>''' | |||
**Study design: Phase II trial | |||
**55 patients with pure testicular seminoma after radical orchiectomy with isolated retroperitoneal lymphadenopathy 1-3 cm in greatest dimension. | |||
***No more than 2 lymph nodes could be enlarged radiographically and lymph nodes needed to be within the ipsilateral RPLND template | |||
***Lymph node enlargement could be synchronous (stage IIA or IIB) or metachronous (stage I with recurrence). | |||
***Open RPLND was performed by certified surgeons who performed ≥8 open RPLND surgeries in the year before site initiation or at least 25 open RPLND surgeries with the past 3 years | |||
**Primary outcome: 2-year relapse-free survival | |||
**Results | |||
***Median follow-up after RPLND: 33 months | |||
***In post-RPLND follow-up, one patient received a single cycle of carboplatin for pN2, all other patients were managed with surveillance | |||
***Pathological nodal stage | |||
****pN0: 16% | |||
****pN1: 22% | |||
****pN2: 56% | |||
****pN3: 5% | |||
***2-year relapse-free survival: 81% (86% cN1 vs. 64% cN2, p=0.04) | |||
***2-year overall survival: 100% | |||
**[https://pubmed.ncbi.nlm.nih.gov/36913642/ Daneshmand, Siamak, et al.] "Surgery in Early Metastatic Seminoma: A Phase II Trial of Retroperitoneal Lymph Node Dissection for Testicular Seminoma With Limited Retroperitoneal Lymphadenopathy." ''Journal of Clinical Oncology'' (2023): JCO-22. | |||
===== CSIIC and III seminoma ===== | ===== CSIIC and III seminoma ===== | ||
| Line 740: | Line 793: | ||
===== Special scenarios ===== | ===== Special scenarios ===== | ||
====== Residual masses after chemotherapy for seminoma ====== | |||
* '''After first-line chemotherapy, 60-80% of patients have radiologically detectable residual masses.''' | |||
* '''<span style="color:#ff0000">Histology of residual masses:</span>''' | |||
** '''<span style="color:#ff0000">Necrosis 90%</span>''' | |||
** '''<span style="color:#ff0000">Viable malignancy: 10%</span>''' | |||
** '''Compared to NSGCT, residual masses after chemotherapy are much more likely to be necrosis (for NSGCT, histology of post-chemotherapy residual masses: necrosis in 40%, viable disease in 15%, and teratoma in 45% (see below)).''' | |||
* '''<span style="color:#ff0000">Management</span>''' | |||
** '''<span style="color:#ff0000">In seminoma, most residual masses do not need to be treated.</span>''' | |||
*** '''Spontaneous resolution of post-chemotherapy residual masses is reported in 50-60% of cases, and the median time to resolution is 13-18 months.''' | |||
*** <span style="color:#ff0000">'''Post-chemotherapy surgery for seminoma is technically difficult'''</span> (and frequently not feasible) because of the desmoplastic reaction that occurs after chemotherapy with resultant increased perioperative morbidity. | |||
*** Teratoma and malignant transformation are much less of a concern with advanced seminoma. | |||
** '''<span style="color:#ff0000">If residual masses > 3 cm, evaluate further with FDG-PET</span>''' | |||
*** '''<span style="color:#ff0000">If FDG-PET positive: post-chemotherapy surgery</span>''' | |||
*** '''<span style="color:#ff0000">If FDG-PET negative: observation.</span>''' | |||
** '''<span style="color:#ff0000">If residual masses< 3 cm: observation.</span>''' | |||
** Post-chemotherapy radiotherapy has no role in the management of residual masses | |||
====== Residual masses after radiotherapy for seminoma ====== | ====== Residual masses after radiotherapy for seminoma ====== | ||
| Line 745: | Line 815: | ||
* '''Patients should undergo biopsy and histologic confirmation of the suspected lesion before management decisions are made.''' | * '''Patients should undergo biopsy and histologic confirmation of the suspected lesion before management decisions are made.''' | ||
** '''Although rare, seminoma may transform into NSGCT elements, and this should be considered in patients with metastatic seminoma who fail to respond to conventional therapy.''' | ** '''Although rare, seminoma may transform into NSGCT elements, and this should be considered in patients with metastatic seminoma who fail to respond to conventional therapy.''' | ||
** Either an open or a laparoscopic biopsy of the para-aortic mass is an acceptable approach if CT-guided biopsy is not feasible or the result is | ** Either an open or a robotic/laparoscopic biopsy of the para-aortic mass is an acceptable approach if CT-guided biopsy is not feasible or the result is non-diagnostic. | ||
** RPLND should not be performed without histologic confirmation of NSGCT pathology. | ** RPLND should not be performed without histologic confirmation of NSGCT pathology. | ||
====== Relapse of seminoma ====== | ====== Relapse of seminoma ====== | ||
| Line 780: | Line 832: | ||
===== CSIA and IB NSGCT ===== | ===== CSIA and IB NSGCT ===== | ||
* '''Options:''' | * '''<span style="color:#ff0000">Options:</span>''' | ||
*# '''Surveillance''' | *# '''<span style="color:#ff0000">Surveillance</span>''' | ||
*# '''Adjuvant primary RPLND''' | *# '''<span style="color:#ff0000">Adjuvant primary RPLND</span>''' | ||
*# '''Adjuvant primary chemotherapy (BEPx1-2)''' | *# '''<span style="color:#ff0000">Adjuvant primary chemotherapy (BEPx1-2)</span>''' | ||
* | *#* '''Newer guidelines, such as 2019 AUA guidelines, recommend 1 cycle for CSIA and 2 cycles for CSIB''' | ||
* | *#* '''2010 CUA Consensus Statement: BEPx2''' | ||
** Long-term survival approaches 100% for each | ** Long-term survival approaches 100% for each | ||
** '''Guidelines''': | ** '''Guidelines''': | ||
*** '''2010 CUA Consensus Statement: surveillance preferred for all CSI NSGCT''' | *** '''2010 CUA Consensus Statement: surveillance preferred for all CSI NSGCT''' | ||
*** '''2019 AUA Guidelines:''' | *** '''<span style="color:#ff0000">2019 AUA Guidelines:</span>''' | ||
**** '''CSIA NSGCT: surveillance recommended''' | **** '''<span style="color:#ff0000">CSIA NSGCT: surveillance recommended</span>''' | ||
**** '''CSIB NSGCT: all options are recommended''' | **** '''<span style="color:#ff0000">CSIB NSGCT: all options are recommended</span>''' | ||
**** '''RPLND is recommended if there is any secondary somatic malignancy (e.g. rhabdomyosarcoma, adenocarcinoma, or primitive neuroectodermal tumor) in the primary tumor''' | **** '''<span style="color:#ff0000">RPLND is recommended if there is any secondary somatic malignancy (e.g. rhabdomyosarcoma, adenocarcinoma, or primitive neuroectodermal tumor) in the primary tumor</span>''' | ||
* '''Surveillance for clinical stage I NSGCT''' | * '''<span style="color:#ff0000">Surveillance for clinical stage I NSGCT</span>''' | ||
** 70-80% of patients with clinical stage I seminoma achieve cure with radical orchiectomy alone | ** 70-80% of patients with clinical stage I seminoma achieve cure with radical orchiectomy alone | ||
** '''Risk factors for relapse on surveillance (2):''' | ** '''<span style="color:#ff0000">Risk factors for relapse on surveillance (2):</span>''' | ||
**# '''Pre-dominant embryonal carcinoma''' | **# '''<span style="color:#ff0000">Pre-dominant embryonal carcinoma</span>''' | ||
**# '''Lymphovascular invasion''' | **# '''<span style="color:#ff0000">Lymphovascular invasion</span>''' | ||
*** The definition of EC predominance in the literature varies from 45-90%. | *** The definition of EC predominance in the literature varies from 45-90%. | ||
*** Other identified risk factors include advanced pT stage, absence of mature teratoma, absence of yolk sac tumor, presence of EC (regardless of the percent composition), percentage of MIB-1 staining, tumor size, and patient age. | *** Other identified risk factors include advanced pT stage, absence of mature teratoma, absence of yolk sac tumor, presence of EC (regardless of the percent composition), percentage of MIB-1 staining, tumor size, and patient age. | ||
| Line 824: | Line 876: | ||
**#* The risk of late toxicity from 2 cycles of chemotherapy is poorly defined, although there appears to be no safe lower limit. | **#* The risk of late toxicity from 2 cycles of chemotherapy is poorly defined, although there appears to be no safe lower limit. | ||
**# Exposes patients to the potential for chemoresistant and/or late relapse | **# Exposes patients to the potential for chemoresistant and/or late relapse | ||
** | **#* Although primary chemotherapy is associated with the lowest risk of relapse, these relapses are less amenable to salvage therapy because they are chemoresistant, particularly if they have received a regimen other than standard dose BEP. In contrast, patients who relapse after RPLND or on surveillance are chemotherapy-naive and are cured with chemotherapy in virtually all cases. | ||
===== CSIS NSGCT ===== | ===== CSIS NSGCT ===== | ||
* '''Defined as the presence of elevated serum tumor markers after orchiectomy without clinical or radiographic evidence of metastatic disease.''' | * '''<span style="color:#ff0000">Defined as the presence of elevated serum tumor markers after orchiectomy without clinical or radiographic evidence of metastatic disease.</span>''' | ||
* '''Should''' be treated similarly to patients with CS IIC and III and '''receive induction chemotherapy according to IGCCCG classification.''' | * '''Should''' be treated similarly to patients with CS IIC and III and '''receive <span style="color:#ff0000">induction chemotherapy according to IGCCCG classification.</span>''' | ||
===== CS IIA and IIB NSGCT ===== | ===== CS IIA and IIB NSGCT ===== | ||
* '''CSIIA with positive markers or CSIIB regardless of markers: primary chemotherapy (recommended by both CUA and AUA)''' | * '''<span style="color:#ff0000">CSIIA with positive markers or CSIIB regardless of markers: primary chemotherapy (recommended by both CUA and AUA)</span>''' | ||
** CUA: Elevated AFP or hCG levels after orchiectomy or bulky lymph nodes (>3cm) are risk factors for recurrence after primary RPLND. Therefore, patients with CS IIA and IIB NSGCT and elevated AFP or hCG levels or bulky lymph nodes (>3 cm) should receive induction chemotherapy. | ** CUA: Elevated AFP or hCG levels after orchiectomy or bulky lymph nodes (>3cm) are risk factors for recurrence after primary RPLND. Therefore, patients with CS IIA and IIB NSGCT and elevated AFP or hCG levels or bulky lymph nodes (>3 cm) should receive induction chemotherapy. | ||
** AUA: Clinicians may offer RPLND as an alternative to chemotherapy to select patients with clinical stage IIB NSGCT with normal post-orchiectomy serum AFP and hCG. | ** AUA: Clinicians may offer RPLND as an alternative to chemotherapy to select patients with clinical stage IIB NSGCT with normal post-orchiectomy serum AFP and hCG. | ||
* '''CSIIA disease without marker elevation''' | * '''<span style="color:#ff0000">CSIIA disease without marker elevation</span>''' | ||
** Substantial proportion of men with clinical stage IIA NSGCT are over-staged | ** Substantial proportion of men with clinical stage IIA NSGCT are over-staged | ||
** Minority of men with clinical stage IIA are upstaged to pathological stage IIB and may be advised to receive two cycles of adjuvant chemotherapy | ** Minority of men with clinical stage IIA are upstaged to pathological stage IIB and may be advised to receive two cycles of adjuvant chemotherapy | ||
** '''CUA: RPLND (with or without adjuvant chemotherapy) or surveillance with surgery for stable or growing lesions (if becomes marker positive use primary chemotherapy)''' | ** '''<span style="color:#ff0000">CUA: RPLND (with or without adjuvant chemotherapy) or surveillance with surgery for stable or growing lesions (if becomes marker positive use primary chemotherapy)</span>''' | ||
** '''AUA: RPLND or chemotherapy''' | ** '''AUA: RPLND or chemotherapy''' | ||
* '''Management after primary RPLND for NSGCT based on pathology (2021 NCCN''' TEST-10'''/2019 AUA):''' | * '''Management after primary RPLND for NSGCT based on pathology (2021 NCCN''' TEST-10'''/2019 AUA):''' | ||
| Line 847: | Line 899: | ||
** '''pN3: chemotherapy''' (BEP x3 or EP x4) | ** '''pN3: chemotherapy''' (BEP x3 or EP x4) | ||
** '''pN1-3 pure teratoma: surveillance''' | ** '''pN1-3 pure teratoma: surveillance''' | ||
** '''Immediate vs. deferred chemotherapy for pathological stage II disease after primary RPLND''' | ** '''<span style="color:#ff00ff">Immediate vs. deferred chemotherapy for pathological stage II disease after primary RPLND</span>''' | ||
*** Population: 195 males found to have positive nodes, (pathologically stage II) after primary RPLND (in whom the procedure was indicated). Nodes had to be considered completely resected and tumor markers had to be normal after primary RPLND. | *** Population: 195 males found to have positive nodes, (pathologically stage II) after primary RPLND (in whom the procedure was indicated). Nodes had to be considered completely resected and tumor markers had to be normal after primary RPLND. | ||
*** Randomized to immediate vs. delayed chemotherapy (cisplatin/vinblastine/bleomycin +/- dactinomycin/cyclophosphamide) | *** Randomized to immediate vs. delayed chemotherapy (cisplatin/vinblastine/bleomycin +/- dactinomycin/cyclophosphamide) | ||
| Line 856: | Line 908: | ||
**** Death from all causes: 5 immediate vs. 3 delayed chemotherapy | **** Death from all causes: 5 immediate vs. 3 delayed chemotherapy | ||
*** Conclusions: immediate chemotherapy in patients found to have pathological stage II after primary RPLND reduces risk of relapse, but no significant difference in cancer-specific or overall survival (though really few deaths) | *** Conclusions: immediate chemotherapy in patients found to have pathological stage II after primary RPLND reduces risk of relapse, but no significant difference in cancer-specific or overall survival (though really few deaths) | ||
*** Williams, Stephen D., et al."Immediate adjuvant chemotherapy versus observation with treatment at relapse in pathological stage II testicular cancer." ''New England Journal of Medicine'' 317.23 (1987): 1433-1438. | *** Williams, Stephen D., et al. "[https://pubmed.ncbi.nlm.nih.gov/2446132/ Immediate adjuvant chemotherapy versus observation with treatment at relapse in pathological stage II testicular cancer.]" ''New England Journal of Medicine'' 317.23 (1987): 1433-1438. | ||
* '''Disadvantage of chemotherapy for metastatic NSGCT''' | * '''Disadvantage of chemotherapy for metastatic NSGCT''' | ||
*# '''Teratoma is resistant to chemotherapy''' | *# '''Teratoma is resistant to chemotherapy''' | ||
** '''RPLND is preferred as initial therapy in patients at risk for retroperitoneal teratoma who are at otherwise low risk for systemic disease''' (normal serum tumor markers, lymphadenopathy <3 cm). | ** '''RPLND is preferred as initial therapy in patients at risk for retroperitoneal teratoma who are at otherwise low risk for systemic disease''' (normal serum tumor markers, lymphadenopathy <3 cm). | ||
** Unresected teratoma has the potential to exhibit rapid growth (growing teratoma syndrome), undergo malignant transformation, or cause late relapse, all of which may have lethal consequences. | ** Unresected teratoma has the potential to exhibit rapid growth (growing teratoma syndrome), undergo malignant transformation, or cause late relapse, all of which may have lethal consequences. | ||
* '''Growing teratoma syndrome''' | * '''<span style="color:#ff0000">Growing teratoma syndrome</span>''' | ||
** '''Should be considered if there is an expected tumour marker decline during chemotherapy but the metastases are growing radiologically''' | ** '''<span style="color:#ff0000">Should be considered if there is an expected tumour marker decline during chemotherapy but the metastases are growing radiologically</span>''' | ||
** '''Management''' | ** '''<span style="color:#ff0000">Management</span>''' | ||
*** '''2010 CUA Guidelines: In most cases, the full course of chemotherapy should be completed and resection of the growing and residual masses should be done post-chemotherapy.''' | *** '''<span style="color:#ff0000">2010 CUA Guidelines: In most cases, the full course of chemotherapy should be completed and resection of the growing and residual masses should be done post-chemotherapy.</span>''' | ||
**** Very rarely, rapid radiological progression in the setting of decreasing tumour marker decline is seen which would necessitate surgical resection prior to the completion of chemotherapy. | **** Very rarely, rapid radiological progression in the setting of decreasing tumour marker decline is seen which would necessitate surgical resection prior to the completion of chemotherapy. | ||
***** Similar description in 2018 AUA Update on on Medical and Surgical Management of Advanced Testis Cancer | ***** Similar description in 2018 AUA Update on on Medical and Surgical Management of Advanced Testis Cancer | ||
| Line 891: | Line 943: | ||
** If the mass was retroperitoneal, a full bilateral template RPLND should be performed. | ** If the mass was retroperitoneal, a full bilateral template RPLND should be performed. | ||
** '''<span style="color:#ff0000">PC-RPLND in NSGCT</span>''' | ** '''<span style="color:#ff0000">PC-RPLND in NSGCT</span>''' | ||
*** '''<span style="color:#ff0000">Distribution of histology | *** '''<span style="color:#ff0000">Distribution of histology[https://pubmed.ncbi.nlm.nih.gov/2478726/]</span>:''' | ||
***# '''<span style="color:#ff0000">Necrosis/fibrosis (≈40%)</span>''' | ***# '''<span style="color:#ff0000">Necrosis/fibrosis (≈40%)</span>''' | ||
***# '''<span style="color:#ff0000">Teratoma (≈45%)</span>''' | ***# '''<span style="color:#ff0000">Teratoma (≈45%)</span>''' | ||
| Line 904: | Line 956: | ||
* '''<span style="color:#ff0000">FDG-PET has NO role in the assessment of patients with NSGCT and residual masses after chemotherapy</span>''' | * '''<span style="color:#ff0000">FDG-PET has NO role in the assessment of patients with NSGCT and residual masses after chemotherapy</span>''' | ||
* '''Patients with residual masses at multiple anatomic sites (retroperitoneum, chest, and left supraclavicular fossa are the most common) and normal tumour markers should undergo resection of all sites of measurable residual disease.''' | * '''Patients with residual masses at multiple anatomic sites (retroperitoneum, chest, and left supraclavicular fossa are the most common) and normal tumour markers should undergo resection of all sites of measurable residual disease.''' | ||
** '''RPLND should be performed before post-chemotherapy surgery at other sites because the probability of residual disease in the retroperitoneum is highest, and RPLND histology is a strong predictor of histology at other sites.''' | ** '''RPLND should be performed before post-chemotherapy surgery at other sites because the probability of residual disease in the retroperitoneum is highest, and RPLND histology is a strong predictor of histology at other sites.''' Therefore, if no disease in retroperitoneum, unlikely to have any disease elsewhere. | ||
*** If RPLND histology shows | *** If RPLND histology shows | ||
**** Viable malignancy, then patient should undergo chemotherapy | **** Viable malignancy, then patient should undergo chemotherapy | ||
| Line 934: | Line 986: | ||
** '''Chemotherapy''' | ** '''Chemotherapy''' | ||
*** '''Cisplatin is associated with fatigue, myelosuppression, infection, peripheral neuropathy, hearing loss, diminished renal function, and death.''' | *** '''Cisplatin is associated with fatigue, myelosuppression, infection, peripheral neuropathy, hearing loss, diminished renal function, and death.''' | ||
***'''Etoposide is associated with myelosuppression''' | |||
** '''Radiation''' | ** '''Radiation''' | ||
*** '''Associated fatigue, nausea and vomiting, leukopenia, and dyspepsia''' | *** '''Associated fatigue, nausea and vomiting, leukopenia, and dyspepsia''' | ||
* '''Late toxicity''' | * '''<span style="color:#ff0000">Late toxicity</span>''' | ||
** '''Hypogonadism''' | ** '''<span style="color:#ff0000">Hypogonadism</span>''' | ||
*** Occurs in | *** Occurs in | ||
**** 10-20% of patients treated with orchiectomy alone | **** 10-20% of patients treated with orchiectomy alone | ||
| Line 943: | Line 996: | ||
**** 20-25% of patients treated with first-line chemotherapy regimens | **** 20-25% of patients treated with first-line chemotherapy regimens | ||
*** Serum AM testosterone and luteinizing hormone levels should be measured in patients with signs and symptoms of hypogonadism | *** Serum AM testosterone and luteinizing hormone levels should be measured in patients with signs and symptoms of hypogonadism | ||
** '''Infertility''' | ** '''<span style="color:#ff0000">Infertility''' | ||
*** Most males are able to have biological children after treatment for GCT but paternity rates are lower for men treated with radiation therapy and/or chemotherapy | *** Most males are able to have biological children after treatment for GCT but paternity rates are lower for men treated with radiation therapy and/or chemotherapy | ||
** '''Cardiovascular disease''' | ** '''<span style="color:#ff0000">Cardiovascular disease</span>''' | ||
*** Risk increased with either subdiaphragmatic radiation or platinum-based chemotherapy | *** Risk increased with either subdiaphragmatic radiation or platinum-based chemotherapy | ||
*** Patients should establish regular care with a primary care physician so that modifiable risk factors for cardiovascular disease (e.g., diet, exercise, smoking, serum lipid levels, blood pressure, serum glucose) can be monitored. | *** Patients should establish regular care with a primary care physician so that modifiable risk factors for cardiovascular disease (e.g., diet, exercise, smoking, serum lipid levels, blood pressure, serum glucose) can be monitored. | ||
** '''Secondary malignancy''' | ** '''<span style="color:#ff0000">Secondary malignancy</span>''' | ||
*** Risk increased with either subdiaphragmatic radiation or platinum-based chemotherapy | *** Risk increased with either subdiaphragmatic radiation or platinum-based chemotherapy | ||
*** Patients should establish regular care with a primary care physician for appropriate health care maintenance and cancer screening as appropriate. | *** Patients should establish regular care with a primary care physician for appropriate health care maintenance and cancer screening as appropriate. | ||
** '''Chemotherapy specific''' | ** '''<span style="color:#ff0000">Chemotherapy specific''' | ||
*** '''Bleomycin | *** '''<span style="color:#ff0000">Bleomycin''' | ||
*** '''Cisplatin | ****'''<span style="color:#ff0000">Pulmonary complications (including pulmonary fibrosis)''' | ||
*** ''' | ****'''<span style="color:#ff0000">Raynaud phenomenon''' | ||
****'''Mild myelosuppressive effects at high doses.''' | |||
*** '''<span style="color:#ff0000">Cisplatin''' | |||
****'''<span style="color:#ff0000">Nephrotoxicity''' | |||
****'''<span style="color:#ff0000">Neurotoxicity''' | |||
****'''<span style="color:#ff0000">Peripheral neuropathy''' | |||
****'''<span style="color:#ff0000">Hearing loss''' | |||
== Special scenarios == | == Special scenarios == | ||
=== <span style="color:#ff0000">Brain metastases</span> === | |||
* '''<span style="color:#ff0000">Associated with choriocarcinoma; should be suspected in any patient with a very high serum hCG level</span>''' | |||
** '''Choriocarcinomas are highly vascular and tend to hemorrhage during chemotherapy, with death rates of 4-10% secondary to intracranial hemorrhage''' | |||
* Management | |||
** Brain metastases at diagnosis: BEP×4 chemotherapy followed by resection of residual masses. | |||
** Relapse in the brain after first-line chemotherapy: second-line chemotherapy followed by resection and/or radiation therapy | |||
*** Relapse in the brain after achieving a complete response to chemotherapy have a worse prognosis than patients with brain involvement at diagnosis. | |||
=== <span style="color:#ff0000">Primary extra-gonadal GCTs</span> === | |||
* '''<span style="color:#ff0000">Site of origin of GCTs: gonadal (95%) vs. extra-gonadal (5%)</span>''' | |||
* '''<span style="color:#ff0000">Develop in midline anatomic locations</span>''' | |||
** '''<span style="color:#ff0000">Most common sites (descending order) of origin: mediastinum, retroperitoneum,</span>''' sacrococcygeal region, and pineal gland, although many unusual sites have also been reported [SASP 2014] | |||
** '''Primary mediastinal GCT''' | |||
*** '''NSGCT''' | |||
**** '''Compared to NSGCTs originating in the testicle or retroperitoneum, primary mediastinal NSGCTs are (4):''' | |||
****# '''More likely to have yolk sac tumour components and be associated with elevated AFP''' | |||
****# '''Associated with Klinefelter syndrome''' | |||
****# '''Less sensitive to chemotherapy''' | |||
****# '''Associated with a poor prognosis''' | |||
*** '''Seminoma''' | |||
**** '''Primary mediastinal seminomas have similar prognosis to testicular seminomas''' | |||
** '''Primary retroperitoneal GCT''' | |||
*** '''Behave similarly to testicular GCTs and carry the same prognosis.''' | |||
* Of patients with metastatic GCT without a testis mass: | |||
** 1/3 definitively have a primary extra-gonadal GCT | |||
** 1/3 have ITGCN in the testis | |||
** 1/3 have sonographic evidence of a “burned-out” primary tumor | |||
* '''Diagnosis and evaluation''' | |||
** '''If midline mass in male age < 40, consider GCT''' | |||
*** Midline mass in male age < 40 with elevated AFP and/or hCG is diagnostic of GCT, even if testicular evaluation is normal; histologic confirmation by biopsy is unnecessary before starting treatment | |||
*** Midline mass in male age < 40 with normal serum tumor markers, perform biopsy of the midline mass to confirm the diagnosis before beginning treatment | |||
* '''Management''' | |||
** '''Inguinal orchiectomy''' | |||
*** '''Indications in patients with suspected extra-gonadal GCT (2):''' | |||
**# '''Pattern of metastasis is consistent with a right-sided or left-sided testicular primary tumor''' | |||
* '''Small (<10 mm), impalpable intratesticular lesions in the absence of disseminated GCT or elevated serum tumor markers | **# '''Sonographic evidence of a “burned-out” primary tumor''' | ||
=== Small (<10 mm), impalpable intratesticular lesions === | |||
*'''Small (<10 mm), impalpable intratesticular lesions in the absence of disseminated GCT or elevated serum tumor markers are a diagnostic dilemma''' | |||
* '''<span style="color:#ff0000">Most of these lesions are benign (testicular cysts, small infarcts, or small Leydig cell or Sertoli cell tumors), however, 20-50% may represent small GCTs (usually seminomas).</span>''' | |||
** '''Risk of malignancy increases with the size of the lesion.''' | |||
* '''Management options (3):''' | |||
*# '''Inguinal orchiectomy''' | |||
*# '''Testis-sparing surgery involving inguinal exploration and excision (with frozen-section analysis to rule out GCT)''' | |||
*#* '''Intraoperative ultrasonography is useful during surgical exploration of the testis to locate the lesion.''' | |||
*# '''Close observation with serial ultrasound scans (with exploration of growing lesions).''' | |||
== Questions == | == Questions == | ||
Latest revision as of 07:38, 23 April 2024
Background[edit | edit source]
- Testicular tumours are classified as Germ Cell Tumours (GCTs) vs. non-GCTs
- 95% of testicular tumours are GCTs
- 5% of testicular tumours are non-germ cell tumours such as sex-cord stromal tumours, adenocarcinoma of the rete testis, and lymphoma
- 95% of GCTs originate in the testicle
- 5% of GCTs originate outside the testicle i.e. primary extra-gonadal GCT (see below)
Epidemiology[edit | edit source]
Incidence[edit | edit source]
- Relatively rare
- Estimated annual incidence
- Age
- Most common malignancy among males aged 20-39 years old[3]
Mortality[edit | edit source]
- Estimated annual mortality
Risk Factors[edit | edit source]
- Inherited (3):
- Family history of GCT
- Germ Cell Neoplasia In-Situ (GCNIS)
- Previously referred to as intratubular germ cell neoplasia (ITGCN) unclassified
- All adult invasive GCTs arise from GCNIS, except spermatocytic seminoma.
- Among males with GCNIS, the risk of developing invasive GCT is ≈50% at 5 years
- GCNIS develops before birth from an arrested gonocyte
- Race
- Caucasian risk > African-American
- Acquired (2):
- Cryptorchidism
- Ipsilateral testis: relative risk 4-6x; relative risk decreases to 2-3x if orchidopexy is performed before puberty
- Contralateral testis: slightly increased risk (relative risk 1.74x)
- Personal history of GCT
- Cryptorchidism
Genetics[edit | edit source]
- Increased number of copies of genetic material from the short arm of chromosome 12 is a universal finding in testicular and extra-gonadal germ cell tumors.
Pathology[edit | edit source]
Classification[edit | edit source]
- Pathological: GCNIS-derived vs. non-GCNIS-derived[7]
- Clinical: seminoma vs. non-seminoma GCT (NSGCT)
- GCTs that contain both seminoma and NSGCT subtypes are classified as NSGCTs
- Clinical classification is based on differences in management and outcome
Seminoma[edit | edit source]
- Most common type of GCT
- Comprises 52-56% of all GCTs (NSGCT comprises 44-48%)
- Occurs at an older average age than NSGCTs
- Most seminoma cases diagnosed in the 4th-5th decade of life
- Arises from GCNIS and is considered to be the common precursor for the other NSGCT subtypes
Non-seminoma[edit | edit source]
- Subtypes (4):
- Embryonal carcinoma (EC)
- Aggressive; associated with a high rate of metastasis, often in the context of normal serum tumor markers
- Most undifferentiated cell type of NSGCT, with totipotential capacity to differentiate to other NSGCT cell types (including teratoma) within the primary tumor or at metastatic sites.
- Choriocarcinoma
- Rare
- Aggressive
- Commonly spreads by hematogenous routes
- Typically manifests with extremely highly elevated serum hCG levels
- Yolk sac tumour
- Almost always produce AFP but not hCG
- Teratoma
- Histologically benign tumors
- Contain well-differentiated or incompletely differentiated elements of at least 2/3 germ cell layers: endoderm, mesoderm, and ectoderm.
- No clinical significance to the distinction between mature and immature teratomas, and histopathologists do not typically distinguish between the two entities.
- Generally associated with normal serum tumor markers, but may cause mildly elevated AFP
- Resistant to chemotherapy
- Rarely, may transform into a somatic malignancy (also known as teratoma with malignant transformation) such as rhabdomyosarcoma, adenocarcinoma, or primitive neuroectodermal tumor
- Histologically benign tumors
- Embryonal carcinoma (EC)
Spermatocytic seminoma[edit | edit source]
- Accounts for <1% of GCTs.
- Believed to have a different pathogenesis and separate cell of origin than classic seminoma
- Does not arise from GCNIS, not associated with a history of cryptorchidism or bilaterally, does not demonstrate i(12p), and does not occur as part of mixed GCTs
- Benign tumor; almost always cured with orchiectomy
Natural history[edit | edit source]
- Rapidly growing tumours
Metastasis[edit | edit source]
Sites of metastasis[edit | edit source]
- Lymph nodes
- Retroperitoneal lymph nodes
- Most common site of metastasis
- 70-80% of GCT metastasis occurs by lymphatic spread from the primary tumor to the retroperitoneal lymph nodes and subsequently to distant sites.
- Exception: choriocarcinoma, with a propensity for hematogenous dissemination.
- 70-80% of GCT metastasis occurs by lymphatic spread from the primary tumor to the retroperitoneal lymph nodes and subsequently to distant sites.
- Most common site of metastasis
- Supraclavicular lymph nodes
- Mediastinal lymph nodes
- Inguinal lymph nodes in patients with previous scrotal violation
- Retroperitoneal lymph nodes
- Visceral
- Lung
- Second most common site of metastasis
- Most common site of visceral metastases
- Pulmonary metastases of testicular GCT represents disease spread via the hematogenous route, whereas mediastinal and cervical metastases represent lymphatic spread.
- Thoracic metastasis in the absence of retroperitoneal disease and/or elevated serum tumor markers is uncommon
- Liver
- Lung
- At the time of diagnosis, metastasis (regional or distant) is present in 33% of cases of NSGCT and 15% of cases of pure seminoma
Diagnosis and Evaluation[edit | edit source]
- Mandatory investigations in a patient with unilateral or bilateral scrotal mass suspicious for testicular neoplasm:
- History and Physical exam
- Labs (1):
- Serum tumour markers (AFP, hCG, LDH)
- Imaging
- Primary: scrotal US with doppler
- Metastasis:
- Regional: CT abdomen/pelvis
- Distant: CT chest (CXR can be used instead of CT if CS I seminoma)
History and Physical Exam[edit | edit source]
History[edit | edit source]
- Signs and Symptoms
- Most common presentation of testicular cancer: painless scrotal mass
- Symptoms related to metastatic disease (e.g. shortness of breath) are the presenting complaint in 10-20% of patients
Physical exam[edit | edit source]
- Genitourinary
- Palpate for any testicular or extra-testicular masses. Note relative size and consistency of affected and normal contralateral testicle.
- A firm intratesticular mass should be managed as a malignant neoplasm until proven otherwise and should be evaluated further with a scrotal ultrasound scan.
- Differential diagnosis of a scrotal mass (8):
- Painless
- Testicular neoplasm
- Paratesticular neoplasm (benign or malignant)
- Hernia
- Varicocele
- Spermatocele
- Painful
- Torsion
- Hematoma
- Epididymoorchitis
- Painless
- Palpate for any testicular or extra-testicular masses. Note relative size and consistency of affected and normal contralateral testicle.
- Sites of metastases
- Supraclavicular lymph nodes
- Inguinal lymph nodes, if prior inguinal or scrotal surgery
- Gynecomastia
- Occurs in 2% of males with GCT
- Results from elevated serum hCG levels, decreased androgen production, and/or increased estrogen levels
Labs[edit | edit source]
Tumour markers (A YET, B SEC)[edit | edit source]
AFP[edit | edit source]
- At diagnosis, elevated in 50-70% of low-stage (CS I, IIA, and IIB) NSGCT and 60-80% of advanced (CS IIC and III) NSGCT
- Produced by (3):
- Yolk sac
- EC
- Teratoma
- Choriocarcinomas and seminomas do not produce AFP
- Clinical implication: pure seminoma in the primary tumor with an elevated serum AFP should be treated as NSGCT
- Upper limit < 11 ng/mL
- Despite most laboratories considering AFP > 8ng/mL to be abnormally elevated, a proportion of the population may have levels up to 15-25 ng/mL in the absence of any pathology; treatment decisions based solely on “elevated” AFP levels that are stable and <25 ng/mL is discouraged
- Serum half-life: 5-7 days
- Other causes of elevated AFP:
- Non-malignant liver disease (infectious, drug-induced, alcohol-induced, autoimmune)
- Hepatocellular carcinoma
- Cancers of the stomach, pancreas, biliary tract, and lung
- Ataxic telangiectasia
- Hereditary tyrosinemia
- Hereditary persistence of AFP (a congenital alteration in the hepatic nuclear factor binding site of the AFP gene)
β-hCG[edit | edit source]
- At diagnosis, elevated in 20-40% of low-stage NSGCT and 40-60% of advanced NSGCT
- Produced by (3):
- Seminoma (15% of cases)
- EC
- Choriocarcinoma
- Upper limit: <5 mU/mL
- Levels > 10,000 IU/L are usually associated with choriocarcinoma.
- Serum half-life: 24 to 36 hours (2019 AUA Update Peds Testis Tumours says 24-48 hours)
- Other causes of elevated hCG:
- Hypogonadism
- LH will be elevated and can be a cause false-positive elevated hCC due to cross-reactivity of the hCG assay with LH
- Supplemental testosterone decreases LH levels, allowing accurate assessment of hCG levels thereafter[8]
- LH will be elevated and can be a cause false-positive elevated hCC due to cross-reactivity of the hCG assay with LH
- Cancers of the liver, biliary tract, pancreas, stomach, lung, breast, kidney, and bladder.
- The α subunit of hCG is common to several pituitary tumors, and so immunoassays for hCG are directed at the β subunit.
- Cannabis use
- Hypogonadism
LDH[edit | edit source]
- At diagnosis, elevated in ≈20% of low-stage GCT and 20-60% of advanced GCT
- Least relevant and clinically applicable of the tumour markers
- Non-specific marker
- Main use in GCT is in the prognostic (S stage classification) assessment at diagnosis.
- Treatment decisions based solely on LDH elevation in the setting of normal AFP and hCG should be discouraged.
- Normal value 48-115 IU/liter
- Magnitude of LDH elevation correlates with bulk of disease.
- Serum half-life: varies[9]
- LDH is expressed in smooth, cardiac, and skeletal muscles and can be elevated from cancerous (kidney, lymphoma, GI, breast) or non-cancerous conditions (heart failure, anemia, HIV)
Pre-orchiectomy tumour markers[edit | edit source]
- Uses (2):
- Support initial diagnosis
- Should not be used to guide decision making about whether or not to perform a radical orchiectomy because AFP or hCG levels in the normal range do not rule out GCT.
- Interpret tumor marker levels after orchiectomy.
- Essential to know whether persistently elevated post-orchiectomy tumour markers are declining compared to pre-orchiectomy levels by their respective half-lives or not, or whether they are rising, as this impacts subsequent treatment decisions.
- Support initial diagnosis
- Should not be used for clinical staging and risk stratification
- Can lead to over- or under-treatment with resulting excess rates of toxicity or relapse, respectively.
Post-orchiectomy tumour markers[edit | edit source]
- Uses (2):
- Evaluate for metastases in the case of persistently elevated/rising post-orchiectomy tumour markers
- Tumour marker levels should normalize after 4 half-lives[10]
- Serum AFP levels should return to normal levels 20–28 days after effective therapy.
- If borderline elevated (within 3x upper limit of normal) post-orchiectomy markers (AFP and hCG), confirm a rising trend before management decisions are made as false-positive elevations may occur.
- Tumour marker levels should normalize after 4 half-lives[10]
- Evaluate for recurrence during surveillance and after completion of therapy (chemotherapy, radiation, surgery).
- Evaluate for metastases in the case of persistently elevated/rising post-orchiectomy tumour markers
Imaging[edit | edit source]
Local[edit | edit source]
Modality[edit | edit source]
Scrotal ultrasound with doppler[edit | edit source]
- Important to evaluate both testicles given 2% incidence of bilateral GCT
- In cases of bilateral GCT, a metachronous lesion is the most common presentation.
- High-frequency transducers (5 to 10 MHz) can readily identify and distinguish intratesticular lesions a few millimeters in size from extra-testicular pathology
- Indications in the context of suspected GCT (3)
- Scrotal mass
- Suspected metastatic GCT with a normal testicular examination
- A small, impalpable scar or calcification indicates a “burned-out” primary testis tumor.
- If sonographic evidence of intratesticular lesions (discrete nodule, stellate scar, coarse calcification), perform radical orchiectomy because GCNIS and residual teratoma are frequently encountered.
- A small, impalpable scar or calcification indicates a “burned-out” primary testis tumor.
- Suspected primary extra-gonadal GCT
- Males with advanced GCT with normal testes on physical examination and ultrasound scan are considered to have primary extragonadal GCT.
- Patients with normal serum tumor markers (hCG and AFP) and indeterminate findings on physical exam or testicular ultrasound for testicular neoplasm should undergo repeat imaging in 6-8 weeks.
- Imaging findings
- Typical GCT is hypoechoic
- 2 or more discrete lesions may be identified
- INSERT IMAGE
- Testicular microlithiasis
- Unclear significance in the general population
- If no history of GCT, risk of GCT is only increased if an additional established risk factor (see above) is present
- If history of GCT, microlithiasis on ultrasound of the contralateral testis is associated with an increased risk of ITGCN.
- Management
- No further evaluation or screening in incidentally detected microlithiasis
- If established risk factor and testicular microlithiasis, counsel patient about the potential increased risk of GCT, need for periodic self-examination and follow-up with a medical professional
- insert image
- Unclear significance in the general population
MRI[edit | edit source]
- Can be considered an adjunct to scrotal ultrasound in patients with lesions suspicious for benign etiology
- Should not delay orchiectomy in patients in whom malignancy is suspected
Metastasis[edit | edit source]
Regional[edit | edit source]
- Regional lymph nodes comprises (7):
- Inter-aortocaval
- Para-aortic
- Para-caval
- Pre-aortic
- Pre-caval
- Retro-aortic
- Retro-caval
- Modality
- CT abdomen/pelvis with oral and IV contrast
- Most effective imaging modality for regional staging
- MRI
- Alternative to CT
- CT abdomen/pelvis with oral and IV contrast
- Imaging findings
- Retroperitoneal lymph nodes
- Pattern of lymph drainage in the retroperitoneum is from right to left.
- For right testis tumors, the primary drainage site is the inter-aortocaval lymph nodes inferior to the renal vessels, followed by the paracaval and para-aortic nodes.
- For left testis tumors, the primary drainage site is the para-aortic lymph nodes, followed by the inter-aortocaval nodes.
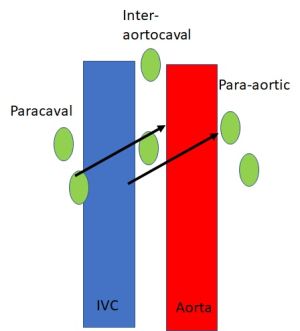
Direction of lymphatic flow in the retroperitoneum
- Pattern of lymph drainage in the retroperitoneum is from right to left.
- "Borderline" retroperitoneal lymph nodes
- Lymph nodes 5-9 mm in the primary landing zone should be viewed with suspicion for regional lymph node metastasis, particularly if they are anterior to the great vessels
- Limitations
- Understaging
- 25-35% of patients with CSI NSGCT and a “normal” CT scan will be found to have pathologically involved retroperitoneal lymph nodes at RPLND
- Overstaging
- 12-40% of patients with CS IIA and IIB disease will be found to have pathologically negative lymph nodes at RPLND
- Understaging
- Retroperitoneal lymph nodes

Distant[edit | edit source]
- Chest
- Timing
- Necessary to complete staging in patients with confirmed GCTs
- Should not delay orchiectomy
- Modality: plain-film chest x-ray vs. CT
- Chest x-ray
- Indications★
- Suspected clinical stage I seminoma; preferred over CT
- When tumor markers are normal, the rate of skip metastasis to the thorax in seminoma is close to 0%, and the addition of CT chest to chest x-ray is very unlikely to alter treatment decisions.
- Suspected clinical stage I seminoma; preferred over CT
- Indications★
- CT scan
- Indications (3)★
- NSGCT
- Skip metastases are more common in non-seminoma than seminoma.
- Elevated and rising post-orchiectomy markers (hCG and AFP)
- Any evidence of metastases on abdominal/pelvic imaging, chest x-ray or physical exam.
- NSGCT
- Indications (3)★
- Chest x-ray
- Timing
- Other
- Bone scan and CT brain
- No role for routine bone scintigraphy or brain CT imaging at the time of diagnosis.★
- In the absence of symptoms or other clinical indicators of disease, visceral metastasis to bone and brain is uncommon in GCT
- Indications for bone scan and CT brain (3):
- Symptoms suggestive of central nervous system or bone involvement
- Poor prognosis disease.
- Highly elevated hCG (>10,000 mU/mL)
- Highly elevated hCG are often associated with metastatic choriocarcinoma, which has a propensity for brain metastases.
- No role for routine bone scintigraphy or brain CT imaging at the time of diagnosis.★
- FDG-PET
- Currently, no role in the routine evaluation of NSGCT and seminoma at the time of diagnosis.
- Bone scan and CT brain
Other[edit | edit source]
- Testicular biopsy: contraindicated
- Scrotal violation increases risk of (2):
- Pelvic or inguinal lymph node metastasis due to altered lymphatic drainage of the testicle
- Local recurrence
- Systematic review of outcomes of scrotal violation in testicular cancer
- Scrotal violation defined at non-standard surgical approaches including trans-scrotal orchiectomy, open testicular biopsy, and fine needle aspiration
- Results
- Median follow-up: 24 to 126 months
- Rate of local recurrence: 2.5% of patients undergoing scrotal violation vs. none of the patients who underwent radical inguinal orchiectomy (P<0.001)
- Among patients undergoing excision of the scrotal scar, 9% had residual, viable GCT.
- No difference in rates of metastatic disease or all-cause mortality based on scrotal violation
- Capelouto, Carl C., et al."Testis cancer: a review of scrotal violation in testicular cancer: is adjuvant local therapy necessary?." The Journal of urology 153.3 (1995): 981-985.
- Scrotal violation increases risk of (2):
Staging[edit | edit source]
TNM (AJCC 8th edition§)[edit | edit source]
T stage (primary tumor)[edit | edit source]
- pTX: cannot be assessed
- pT0: no evidence of primary tumour
- pTis: germ cell neoplasia in situ
- pT1: tumour limited to testis (including rete testis invastion) without lymphovascular invasion (LVI)
- For pure seminoma:
- pT1a: tumour size < 3 cm
- pT1b: tumour size ≥ 3 cm
- For pure seminoma:
- pT2: tumour limited to testis (including rete testis invastion) with LVI or tumour invading hilar soft tissue, epididymis or tunica vaginalis
- pT3: direct (continuous) spermatic cord soft tissue invasion
- LVI of the spermatic cord without soft tissue invasion is not pT3
- pT4: direct scrotum invasion
N Stage (regional lymph node stage)[edit | edit source]
- Clinical
- cNX: regional lymph nodes cannot be assessed
- cN0: no regional lymph node metastasis
- cN1: metastasis with a lymph node mass ≤2 cm in greatest dimension OR multiple lymph nodes, each ≤2 cm cm in greatest dimension
- cN2: metastasis with a lymph node mass >2 cm but ≤5 cm in greatest dimension OR multiple lymph nodes, any one mass >2 cm but ≤5 cm
- cN3: metastasis with a lymph node mass >5 cm in greatest dimension
- Pathologic
- pNX: regional lymph nodes cannot be assessed
- pN0: no regional lymph node metastasis
- pN1: metastasis with a lymph node mass ≤2 cm in greatest dimension AND ≤5 positive nodes, none >2 cm in greatest dimension
- pN2:
- Metastasis with a lymph node mass >2 cm but ≤5 cm in greatest dimension OR
- >5 nodes positive, none >5 cm in greatest dimension OR
- Extranodal extension of tumour
- pN3: metastasis with a lymph node mass >5 cm in greatest dimension
M stage (distant metastasis)[edit | edit source]
- MX: distant metastasis cannot be assessed
- M0: no distant metastasis
- M1a: non-regional lymph node (ex: iliac, inguinal, pelvic NOS) or lung metastasis
- M1b: non-lung visceral metastasis
S stage (serum markers)[edit | edit source]
- SX: serum tumor markers not available or not performed
- S0: markers within normal limits
- S1: LDH < 1.5 x upper limit of normal, hCG < 5,000 mIU/mL and AFP < 1,000 ng/mL
- S2: LDH 1.5 - 10 x upper limit of normal OR hCG 5,000 - 50,000 mIU/mL OR AFP 1,000 - 10,000 ng/mL
- S3: LDH > 10 x upper limit of normal OR hCG > 50,000 mIU/mL OR AFP > 10,000 ng/mL
Clinical staging[edit | edit source]
- Prognosis of GCT and initial management decisions are determined by clinical stage (CS)
- Based on (3):
- Pathologic stage of the primary tumour (pT stage)
- Presence and extent of regional (N stage) and distant metastatic disease (M stage)
- Post-orchiectomy serum tumor marker levels (S stage)
- Serum tumor markers (AFP, hCG, and LDH) should be repeated at appropriate T1/2 time intervals after orchiectomy to determine nadir for staging and risk stratification
- For patients with elevated AFP or hCG post-orchiectomy, clinicians should monitor serum tumor markers to establish nadir levels before treatment only if marker nadir levels would influence treatment.
- Serum tumor markers (AFP, hCG, and LDH) should be repeated at appropriate T1/2 time intervals after orchiectomy to determine nadir for staging and risk stratification
- Testicular cancer clinical stage groups
| Stage grouping | ||||
| Stage 0 | pTis | N0 | M0 | S0 |
| Stage I | pT1-T4 | N0 | M0 | SX |
| Stage IA | pT1 | N0 | M0 | S0 |
| Stage IB | pT2 - pT4 | N0 | M0 | S0 |
| Stage IS | Any pT/TX | N0 | M0 | S1-3 |
| Stage II | Any pT/TX | N1-N3 | M0 | SX |
| Stage IIA | Any pT/TX | N1 | M0 | S0 |
| Any pT/TX | N1 | M0 | S1 | |
| Stage IIB | Any pT/TX | N2 | M0 | S0 |
| Any pT/TX | N2 | M0 | S1 | |
| Stage IIC | Any pT/TX | N3 | M0 | S0 |
| Any pT/TX | N3 | M0 | S1 | |
| Stage III | Any pT/TX | Any N | M1a | SX |
| Stage IIIA | Any pT/TX | Any N | M1a | S0 |
| Any pT/TX | Any N | M1a | S1 | |
| Stage IIIB | Any pT/TX | N1-N3 | M0 | S2 |
| Any pT/TX | Any N | M1a | S2 | |
| Stage IIIC | Any pT/TX | N1-N3 | M0 | S3 |
| Any pT/TX | Any N | M1a | S3 | |
| Any pT/TX | Any N | M1b | Any S |
- Overview of clinical staging:
- Clinical stage (CS) I: disease confined to the testis
- CS II: presence of regional (retroperitoneal) lymph node metastasis
- CS III: non-regional lymph node and/or visceral metastasis, although post-orchiectomy serum tumour marker levels can upstage patients from CSII to CSIII
Management[edit | edit source]
General principles[edit | edit source]
- Any post-pubertal male, regardless of age, should be treated according to adult treatment guidelines.
- Management decisions should be made in a multidisciplinary setting involving experienced clinicians in urology, medical oncology, radiation oncology, pathology, and radiology.
- Review of primary tumor specimens by experienced pathologists is recommended.
- Management decisions should be based on imaging obtained within the preceding 4 weeks and serum tumor markers (hCG and AFP) within the preceding 10 days.
- Due to the rapid growth of many GCT, particularly NSGCT, there is a risk of disease progression between staging studies and intervention. Therefore, risk adapted management decisions (i.e. RPLND for Stage IIA disease) should be made based on recent imaging and serum tumor marker levels to avoid undertreatment.
- In patients with normal serum tumor markers (hCG and AFP) and equivocal imaging findings for metastasis, consider repeat imaging in 6-8 weeks to clarify the extent of disease prior to making a treatment recommendation.
- Prior to definitive management, patients should be counseled about the risks of (3):
- Hypogonadism
- Hormone levels in long-term survivors of testicular cancer
- Population: 1235 patients with history of unilateral orchiectomy for testicular cancer and adjuvant RPLND only, radiotherapy only, or chemotherapy
- Compared to healthy controls
- Results
- Approximately 11 years follow-up
- No significant difference in serum testosterone between testicular cancer patients and healthy controls
- Significantly higher age-adjusted LH in testicular cancer patients
- Nord, Carina, et al. "Gonadal hormones in long-term survivors 10 years after treatment for unilateral testicular cancer." European urology 44.3 (2003): 322-328.
- Over long-term follow-up, up to 10-15% of patients will have low serum testosterone levels or will require testosterone replacement therapy
- Hormone levels in long-term survivors of testicular cancer
- Infertility
- At diagnosis, up to 50% have impaired semen parameters and 10% are azoospermic
- Sperm cryopreservation
- Timing
- Pre-orchiectomy
- Consider in patients without a normal contralateral testicle or with known subfertility
- Post-orchiectomy
- Recommended before treatment (other than orchiectomy) is initiated in patients who are undecided or are planning future paternity.
- Virtually all patients become azoospermic after chemotherapy, and 50-80% of patients with normal semen parameters at diagnosis return to these levels within 2 and 5 years, respectively.
- Recovery of spermatogenesis after radiation therapy for seminoma may take 2-3 years or longer.
- Consider in patients that do not require further treatment with a normal contralateral testicle or known fertility, who are undecided or are planning future paternity, given the potential risk of pathologic process (testicular cancer, trauma) involving the normal contralateral testicle
- Recommended before treatment (other than orchiectomy) is initiated in patients who are undecided or are planning future paternity.
- Pre-orchiectomy
- Timing
- Contralateral tumour
- Patients with a history of GCT or GCNIS should be informed of risks of a second primary tumor, while rare, is significantly increased in the contralateral testis
- Hypogonadism
Orchiectomy[edit | edit source]
- See Orchiectomy Chapter Notes
Radical inguinal orchiectomy[edit | edit source]
- Testicular prosthesis should be discussed prior to orchiectomy.
- Approach: inguinal
- Trans-scrotal orchiectomy: contraindicated due to risks of scrotal violation (see above)
- Patients who have undergone scrotal orchiectomy for malignant neoplasm should be counseled regarding the increased risk of local recurrence and may rarely be considered for adjunctive therapy (excision of scrotal scar or radiotherapy) for local control
- In patients that have received systemic therapy following scrotal orchiectomy, local relapse is rare and adjuvant therapy is not needed
- Patients who have undergone scrotal orchiectomy for malignant neoplasm should be counseled regarding the increased risk of local recurrence and may rarely be considered for adjunctive therapy (excision of scrotal scar or radiotherapy) for local control
- Trans-scrotal orchiectomy: contraindicated due to risks of scrotal violation (see above)
- Patients suspected of having a testicular neoplasm should undergo a radical inguinal orchiectomy with removal of the tumor-bearing testicle and spermatic cord to the level of the internal inguinal ring.
- In very rare cases where there is a possibility of a benign tumour, excisional biopsy with a frozen section should be performed prior to definitive orchiectomy to allow for the possibility of organ-sparing partial orchiectomy.
- Timing
- In general, orchiectomy should be performed prior to any further treatment.
- Exception: in patients with life-threatening metastatic disease and an unequivocally elevated AFP and/or HCG, orchiectomy should not delay the start of chemotherapy and can be postponed until later in the treatment course
- In general, orchiectomy should be performed prior to any further treatment.
Testis-sparing surgery (TSS)[13][edit | edit source]
- Not recommended in patients with a testicular lesion suspicious for malignant neoplasm and a normal contralateral testis; radical inguinal orchiectomy is recommended
- Indications (3)
- Patients wishing to preserve gonadal function
- Mass <2cm
- And one of the following:
- Equivocal ultrasound/physical exam findings and negative tumor markers (hCG and AFP)
- Congenital, acquired or functionally solitary testis
- Bilateral synchronous tumors
- Patients considering TSS should be counseled regarding (5):
- Higher risk of local recurrence
- Need for monitoring with physical examination and ultrasound
- Role of adjuvant radiotherapy to the testicle to reduce local recurrence
- Impact of radiotherapy on sperm and testosterone production
- Risk of testicular atrophy and need for testosterone replacement therapy, and/or subfertility/infertility
- When TSS is performed, in addition to the suspicious mass, multiple biopsies of the ipsilateral testicle normal parenchyma should be obtained for evaluation by an experienced genitourinary pathologist to rule out GCNIS.
- 50-80% undergoing TSS have concomitant GCNIS in the ipsilateral testis
- GCNIS
- Rationale for treatment is based on the high risk of developing invasive GCT.
- Can be diagnosed by testicular biopsy performed for the investigation of infertility, contralateral testis biopsy in patients with GCT, or within the affected testis in a patient undergoing TSS
- Management options
- Orchiectomy
- Low-dose (18-20 Gy) radiotherapy
- Close observation
- If GSCNIS on testis biopsy or malignant neoplasm after TSS are found:
- If patient prioritizes preservation of fertility and testicular androgen production, surveillance is recommended
- For patients with abnormal semen parameters but sufficient for assisted reproductive techniques, close surveillance with periodic ultrasound evaluation of the testis is a reasonable strategy with deferred therapy until successful pregnancy and/or development of GCT.
- If patient prioritizes reduction of cancer risk, testicular radiation (18-20 Gy) or orchiectomy is recommended
- Radiation
- Advantage
- Reduced risk of hypogonadism compared to orchiectomy
- Leydig cells are radioresistant compared with germinal epithelium.
- Leydig cell function may decline over time, and 40% of men who receive radiation therapy require supplemental testosterone
- Reduced risk of hypogonadism compared to orchiectomy
- Disadvantage
- Increased risk of infertility compared to orchiectomy
- For patients with a normal contralateral testis who desire future paternity, radical orchiectomy is preferred because scatter to the contralateral testis from radiotherapy may impair spermatogenesis.
- Radiation at these doses causes permanent sterility of the treated testis, but can be delayed in patients who wish to father children.
- Increased risk of infertility compared to orchiectomy
- Advantage
- Radical orchiectomy
- Advantage
- Most definitive treatment, although low-dose radiotherapy (≥20 Gy) is associated with similar rates of local control with the prospect of preserving testicular endocrine function
- Advantage
- Radiation
- If patient prioritizes preservation of fertility and testicular androgen production, surveillance is recommended
- If GCNIS is not found on biopsy:
- It is highly likely that GCNIS is present outside of the sampled tissue, and the patient should be followed with serial self-testicular exam, ultrasound, and tumor markers as appropriate.
- Any local recurrence within the ipsilateral testis occurring with or without adjuvant therapy should be managed with completion radical orchiectomy
Contralateral testis biopsy[edit | edit source]
- An open inguinal biopsy of the contralateral testis may be considered in patients with risk factors for testicular cancer or patients with suspicious lesions on preoperative ultrasound scan
Delayed orchiectomy[edit | edit source]
- In a small subset of patients with widespread and/or symptomatic GCT, the diagnosis is made based on biopsy of a metastatic lesion or empirically based on clinical and serologic features. In these unique settings, initiation of systemic chemotherapy supersedes diagnostic orchiectomy. Because of high discordance of pathologic response rates within the testicle, a delayed orchiectomy is recommended for all patients with NSGCT after induction chemotherapy, even in the setting of a complete response in the retroperitoneum
- The role of delayed orchiectomy is more controversial in patients with presumed primary retroperitoneal/extragonadal GCT.
- Radical orchiectomy has been advocated when the metastatic pattern of retroperitoneal disease lateralizes to the expected distribution of a testicular primary.
Post-orchiectomy management[edit | edit source]
- Based on histology (seminoma vs. NSGCT) and clinical stage
General principles[edit | edit source]
- Newly elevated and/or rising serum tumor marker levels after orchiectomy indicate the presence of metastatic disease, and these patients should receive induction chemotherapy.
- In the setting of a negative metastatic evaluation and slowly declining markers (i.e., not according to half-life), patients should be monitored closely and have levels checked periodically until the levels normalize or begin to rise.
- Surveillance for clinical stage I disease
- Advantages (1):
- Potentially reducing treatment-related toxicity by restricting treatment to patients with a proven need for it.
- Radical orchiectomy alone has high cure rate in patients with CSI GCT (80-85% for CS I seminoma and 70-80% for CSI NSGCT)
- Patients that relapse on surveillance have excellent outcomes with salvage therapy.
- Radical orchiectomy alone has high cure rate in patients with CSI GCT (80-85% for CS I seminoma and 70-80% for CSI NSGCT)
- Potentially reducing treatment-related toxicity by restricting treatment to patients with a proven need for it.
- Disadvantages (4):
- Highest risk of relapse (compared to adjuvant treatment)
- Need for long-term (>5 years) surveillance
- Risk of second malignant neoplasms owing to intensive surveillance CT imaging
- More intensive therapy required to treat patients at the time of relapse than if they had received treatment at diagnosis
- Advantages (1):
- Radiotherapy
- Seminoma are sensitive to radiation therapy
- Radiation therapy has no role in NSGCT with the exception of treatment for brain metastases.
- Chemotherapy
- International Germ Cell Cancer Collaborative Group (IGCCCG) risk classification
- Used over the TNM system to select the chemotherapy regimen and number of cycles in patients receiving chemotherapy for advanced disease
- Developed in patients with metastatic GCT at the time of diagnosis and is NOT applicable to patients with relapsed GCT
- Classified into (3): good, intermediate, and poor prognosis
- Classification based on:
- NSGCT (3):
- Presence of non-pulmonary visceral metastasis
- Primary mediastinal NSGCT
- TMs at the initiation of chemotherapy (not levels measured before orchiectomy)
- Seminoma (1):
- Presence of non-pulmonary visceral metastasis
- No poor prognosis category
- Presence of non-pulmonary visceral metastasis
- NSGCT (3):
- Used over the TNM system to select the chemotherapy regimen and number of cycles in patients receiving chemotherapy for advanced disease
- International Germ Cell Cancer Collaborative Group (IGCCCG) risk classification
| Histology | Good prognosis | Intermediate prognosis | Poor prognosis (II or greater) |
| Non-seminoma |
|
|
|
| Seminoma |
|
|
- During chemotherapy, patients need to be monitored on a regular basis with serial tumour marker estimation.
- Post-chemotherapy, radiological restaging should be performed in all patients.
- If the expected tumour marker decline is seen, all residual masses should be treated appropriately.
- If the tumour markers plateau and are at a low level, they should be followed closely.
- If there is a persistent plateau or tumour marker decline, residual masses should be treated appropriately.
- Markedly elevated HCG prior to treatment may take longer to normalize or plateau at the end of chemotherapy
- RPLND
- See RPLND Chapter Notes
Seminoma[edit | edit source]
CSIA and IB Seminoma[edit | edit source]
- Options (3):
- Preferred (1): surveillance
- Alternatives (2):
- Adjuvant primary radiotherapy (20 Gy to the para-aortic region)
- Adjuvant primary chemotherapy with single-agent carboplatin (1 cycle)
- Both 2019 AUA and 2010 CUA guidelines recommend surveillance, adjuvant as an alternative
- If adjuvant treatment is chosen
- CUA recommends radiotherapy over chemotherapy
- EAU recommends against radiotherapy
- SWONTECA recommends radiotherapy only if chemotherapy not suitable
- If adjuvant treatment is chosen
- Long-term survival rates approaching 100% for each approach
- Surveillance for clinical stage I seminoma
- 80-85% of patients with clinical stage I seminoma achieve cure with radical orchiectomy alone
- Protocol varies by institution, no consensus
- History and physical examination: every 4-6 months for the first 2 years, and then every 6-12 months in years 3-5.
- Cross-sectional imaging of the abdomen with or without the pelvis: every 4-6 months for the first 2 years, and then every 6-12 months in years 3-5.
- Imaging of the chest and serum tumor marker assessment can be obtained as clinically indicated.
- Compared with NSGCT, surveillance for CS I seminoma is complicated by the limited utility of serum tumor markers to detect relapse
- Risk factors for relapse on surveillance (2):
- Tumor size >4 cm
- Rete testis invasion
- Patients who relapse on surveillance should be fully restaged and treated based on their TNM-s status.
- Adjuvant primary radiotherapy
- Delivered as dog-leg (retroperitoneum and ipsilateral pelvis) vs. para-aortic region
- Dog-leg
- Outcomes
- In-field recurrence after dog-leg radiotherapy occurs in <1%.
- Most common sites of recurrence are the thorax and left supraclavicular fossa.
- Virtually all recurrences are cured with first-line chemotherapy.
- Persistent oligospermia after dog-leg radiotherapy occurs in 8%
- In-field recurrence after dog-leg radiotherapy occurs in <1%.
- Advantage
- Does not require serial follow-up CT imaging after treatment
- Outcomes
- Para-aortic
- Advantage
- Smaller field and dose.
- Disadvantage
- Requires serial follow-up CT imaging after treatment
- Advantage
- Dog-leg vs. para-aortic
- RTC found para-aortic to be non-inferior to dog-leg radiotherapy in CSI seminoma§
- Dog-leg
- Delivered as dog-leg (retroperitoneum and ipsilateral pelvis) vs. para-aortic region
- Adjuvant primary chemotherapy
- Cisplatin is inferior to carboplatin for CSI seminoma
- Patients require serial follow-up CT imaging
CS IIA and IIB Seminoma[edit | edit source]
- ≈15-20% of patients with seminoma have CS II disease at diagnosis; 70% of these patients have CS IIA and IIB.
- CSIIA:
- CUA: Dog-leg radiotherapy (25-35 Gy) preferred over first-line chemotherapy (BEP×3 or EP×4)
- AUA: radiotherapy or chemotherapy
- CSIIB:
- CUA: depending on bulk of disease and location of lymph nodes, radiation or chemotherapy [good risk chemotherapy BEP×3 or EP×4] can be used.
- First-line chemotherapy is recommended for bulky (>3 cm) and/or multifocal retroperitoneal metastases
- AUA:
- CSIIB with lymph node ≤3cm: radiotherapy or chemotherapy
- CSIIB with lymph node >3cm: chemotherapy
- CUA: depending on bulk of disease and location of lymph nodes, radiation or chemotherapy [good risk chemotherapy BEP×3 or EP×4] can be used.
- Routine surveillance CT imaging is unnecessary after complete resolution of disease.
- Surgery in Early Metastatic Seminoma (SEMS) Trial
- Study design: Phase II trial
- 55 patients with pure testicular seminoma after radical orchiectomy with isolated retroperitoneal lymphadenopathy 1-3 cm in greatest dimension.
- No more than 2 lymph nodes could be enlarged radiographically and lymph nodes needed to be within the ipsilateral RPLND template
- Lymph node enlargement could be synchronous (stage IIA or IIB) or metachronous (stage I with recurrence).
- Open RPLND was performed by certified surgeons who performed ≥8 open RPLND surgeries in the year before site initiation or at least 25 open RPLND surgeries with the past 3 years
- Primary outcome: 2-year relapse-free survival
- Results
- Median follow-up after RPLND: 33 months
- In post-RPLND follow-up, one patient received a single cycle of carboplatin for pN2, all other patients were managed with surveillance
- Pathological nodal stage
- pN0: 16%
- pN1: 22%
- pN2: 56%
- pN3: 5%
- 2-year relapse-free survival: 81% (86% cN1 vs. 64% cN2, p=0.04)
- 2-year overall survival: 100%
- Daneshmand, Siamak, et al. "Surgery in Early Metastatic Seminoma: A Phase II Trial of Retroperitoneal Lymph Node Dissection for Testicular Seminoma With Limited Retroperitoneal Lymphadenopathy." Journal of Clinical Oncology (2023): JCO-22.
CSIIC and III seminoma[edit | edit source]
- Regimen and number of cycles are based on IGCCCG risk classification (see above)
- Good-risk: BEP×3 or EP×4
- Intermediate-risk: BEP×4
Special scenarios[edit | edit source]
Residual masses after chemotherapy for seminoma[edit | edit source]
- After first-line chemotherapy, 60-80% of patients have radiologically detectable residual masses.
- Histology of residual masses:
- Necrosis 90%
- Viable malignancy: 10%
- Compared to NSGCT, residual masses after chemotherapy are much more likely to be necrosis (for NSGCT, histology of post-chemotherapy residual masses: necrosis in 40%, viable disease in 15%, and teratoma in 45% (see below)).
- Management
- In seminoma, most residual masses do not need to be treated.
- Spontaneous resolution of post-chemotherapy residual masses is reported in 50-60% of cases, and the median time to resolution is 13-18 months.
- Post-chemotherapy surgery for seminoma is technically difficult (and frequently not feasible) because of the desmoplastic reaction that occurs after chemotherapy with resultant increased perioperative morbidity.
- Teratoma and malignant transformation are much less of a concern with advanced seminoma.
- If residual masses > 3 cm, evaluate further with FDG-PET
- If FDG-PET positive: post-chemotherapy surgery
- If FDG-PET negative: observation.
- If residual masses< 3 cm: observation.
- Post-chemotherapy radiotherapy has no role in the management of residual masses
- In seminoma, most residual masses do not need to be treated.
Residual masses after radiotherapy for seminoma[edit | edit source]
- Patients should undergo biopsy and histologic confirmation of the suspected lesion before management decisions are made.
- Although rare, seminoma may transform into NSGCT elements, and this should be considered in patients with metastatic seminoma who fail to respond to conventional therapy.
- Either an open or a robotic/laparoscopic biopsy of the para-aortic mass is an acceptable approach if CT-guided biopsy is not feasible or the result is non-diagnostic.
- RPLND should not be performed without histologic confirmation of NSGCT pathology.
Relapse of seminoma[edit | edit source]
- If chemo-naïve:
- Patients relapsing on surveillance should receive primary radiotherapy
- Patients with CSI or II seminoma treated with radiotherapy, or those on surveillance that relapse with bulky (>3 cm) retroperitoneal masses and systemic relapse should receive first-line chemotherapy based on ICCCG risk category
- Salvage rates approach 100%.
- If early relapse after chemotherapy: salvage chemotherapy
- An important consideration for patients with advanced seminoma who relapse after first-line chemotherapy is the potential for teratoma at the site of relapse.
- Patients with normal serum tumor markers should undergo biopsy before starting second-line chemotherapy.
NSGCT[edit | edit source]
CSIA and IB NSGCT[edit | edit source]
- Options:
- Surveillance
- Adjuvant primary RPLND
- Adjuvant primary chemotherapy (BEPx1-2)
- Newer guidelines, such as 2019 AUA guidelines, recommend 1 cycle for CSIA and 2 cycles for CSIB
- 2010 CUA Consensus Statement: BEPx2
- Long-term survival approaches 100% for each
- Guidelines:
- 2010 CUA Consensus Statement: surveillance preferred for all CSI NSGCT
- 2019 AUA Guidelines:
- CSIA NSGCT: surveillance recommended
- CSIB NSGCT: all options are recommended
- RPLND is recommended if there is any secondary somatic malignancy (e.g. rhabdomyosarcoma, adenocarcinoma, or primitive neuroectodermal tumor) in the primary tumor
- Surveillance for clinical stage I NSGCT
- 70-80% of patients with clinical stage I seminoma achieve cure with radical orchiectomy alone
- Risk factors for relapse on surveillance (2):
- Pre-dominant embryonal carcinoma
- Lymphovascular invasion
- The definition of EC predominance in the literature varies from 45-90%.
- Other identified risk factors include advanced pT stage, absence of mature teratoma, absence of yolk sac tumor, presence of EC (regardless of the percent composition), percentage of MIB-1 staining, tumor size, and patient age.
- Surveillance protocol varies by institution, no consensus
- History and physical examination: every 2-3 months in year 1, every 2-4 months in year 2, every 4-6 months in year 3, and every 6-12 months for years 4 and 5
- Serum tumor markers (AFP, hCG +/- LDH): every 2-3 months in year 1, every 2-4 months in year 2, every 4-6 months in year 3, and every 6-12 months for years 4 and 5
- Radiologic assessment (chest x-ray and imaging of the abdomen with or without the pelvis): every 3-6 months in year 1 starting at 3 months, every 4-12 months in year 2, once in year 3, and once in year 4 or 5.
- Men at higher risk of relapse (e.g., lymphovascular invasion) should be imaged with shorter intervals.
- >90% of relapses occur within the first 2 years, but late relapses (>5 years) are seen in 1% of patients; after this time, annual serologic and radiographic assessment may be performed as indicated based upon clinical concerns.
- Compared with NSGCT, surveillance for CS I seminoma is needed for a longer period because 10% to 20% of relapses occur 4 years or more after diagnosis.
- Patients who relapse on surveillance should be fully restaged and treated based on their TNM-s status.
- Early and late relapses have similar prognosis
- Adjuvant primary RPLND
- Primary RPLND should be performed with curative (rather than staging) intent in all patients.
- Full, bilateral template dissection is associated with the lowest risk of abdominopelvic recurrence (<2%) and the highest rate of antegrade ejaculation (>90%) when nerve-sparing techniques are employed.
- A multi-center randomized trial comparing primary RPLND to chemotherapy for CS I found that chemotherapy was associated with a lower risk of relapse. The relapse rate after primary RPLND in this trial was 11%, higher than other published series, suggesting that RPLND should be performed in experienced centers.
- Adjuvant primary chemotherapy
- BEP x 1-2 is typically used.
- Advantages (2):
- Highest relapse-free survival with any single treatment modality
- Can be delivered at community-based institutions
- Disadvantages (4):
- Does not treat retroperitoneal teratoma
- Long-term surveillance CT imaging of the retroperitoneum is required
- Potential risk of late toxicity (see below).
- The risk of late toxicity from 2 cycles of chemotherapy is poorly defined, although there appears to be no safe lower limit.
- Exposes patients to the potential for chemoresistant and/or late relapse
- Although primary chemotherapy is associated with the lowest risk of relapse, these relapses are less amenable to salvage therapy because they are chemoresistant, particularly if they have received a regimen other than standard dose BEP. In contrast, patients who relapse after RPLND or on surveillance are chemotherapy-naive and are cured with chemotherapy in virtually all cases.
CSIS NSGCT[edit | edit source]
- Defined as the presence of elevated serum tumor markers after orchiectomy without clinical or radiographic evidence of metastatic disease.
- Should be treated similarly to patients with CS IIC and III and receive induction chemotherapy according to IGCCCG classification.
CS IIA and IIB NSGCT[edit | edit source]
- CSIIA with positive markers or CSIIB regardless of markers: primary chemotherapy (recommended by both CUA and AUA)
- CUA: Elevated AFP or hCG levels after orchiectomy or bulky lymph nodes (>3cm) are risk factors for recurrence after primary RPLND. Therefore, patients with CS IIA and IIB NSGCT and elevated AFP or hCG levels or bulky lymph nodes (>3 cm) should receive induction chemotherapy.
- AUA: Clinicians may offer RPLND as an alternative to chemotherapy to select patients with clinical stage IIB NSGCT with normal post-orchiectomy serum AFP and hCG.
- CSIIA disease without marker elevation
- Substantial proportion of men with clinical stage IIA NSGCT are over-staged
- Minority of men with clinical stage IIA are upstaged to pathological stage IIB and may be advised to receive two cycles of adjuvant chemotherapy
- CUA: RPLND (with or without adjuvant chemotherapy) or surveillance with surgery for stable or growing lesions (if becomes marker positive use primary chemotherapy)
- AUA: RPLND or chemotherapy
- Management after primary RPLND for NSGCT based on pathology (2021 NCCN TEST-10/2019 AUA):
- pN0: surveillance
- pN1: surveillance (preferred) vs. chemotherapy (BEP x2 or EP x2)
- pN2: chemotherapy (BEP x2 or EP x2) (preferred) vs. surveillance
- pN3: chemotherapy (BEP x3 or EP x4)
- pN1-3 pure teratoma: surveillance
- Immediate vs. deferred chemotherapy for pathological stage II disease after primary RPLND
- Population: 195 males found to have positive nodes, (pathologically stage II) after primary RPLND (in whom the procedure was indicated). Nodes had to be considered completely resected and tumor markers had to be normal after primary RPLND.
- Randomized to immediate vs. delayed chemotherapy (cisplatin/vinblastine/bleomycin +/- dactinomycin/cyclophosphamide)
- Results:
- Median follow-up: 4 years
- Relapse rate at 2 years: 6% immediate vs. 49% delayed chemotherapy
- Cancer-specific deaths: 1 immediate vs. 3 delayed chemotherapy
- Death from all causes: 5 immediate vs. 3 delayed chemotherapy
- Conclusions: immediate chemotherapy in patients found to have pathological stage II after primary RPLND reduces risk of relapse, but no significant difference in cancer-specific or overall survival (though really few deaths)
- Williams, Stephen D., et al. "Immediate adjuvant chemotherapy versus observation with treatment at relapse in pathological stage II testicular cancer." New England Journal of Medicine 317.23 (1987): 1433-1438.
- Disadvantage of chemotherapy for metastatic NSGCT
- Teratoma is resistant to chemotherapy
- RPLND is preferred as initial therapy in patients at risk for retroperitoneal teratoma who are at otherwise low risk for systemic disease (normal serum tumor markers, lymphadenopathy <3 cm).
- Unresected teratoma has the potential to exhibit rapid growth (growing teratoma syndrome), undergo malignant transformation, or cause late relapse, all of which may have lethal consequences.
- Growing teratoma syndrome
- Should be considered if there is an expected tumour marker decline during chemotherapy but the metastases are growing radiologically
- Management
- 2010 CUA Guidelines: In most cases, the full course of chemotherapy should be completed and resection of the growing and residual masses should be done post-chemotherapy.
- Very rarely, rapid radiological progression in the setting of decreasing tumour marker decline is seen which would necessitate surgical resection prior to the completion of chemotherapy.
- Similar description in 2018 AUA Update on on Medical and Surgical Management of Advanced Testis Cancer
- Campbell's 11th edition, Chapter 34, page 805: Special mention is made of patients with declining or normalized serum tumor markers during first-line chemotherapy with enlarging (usually cystic) masses. These patients are considered to have growing teratoma syndrome. In these rare cases, chemotherapy is temporarily interrupted, and patients are taken for surgical resection. With complete surgical resection, the long-term prognosis for these patients is favorable
- Very rarely, rapid radiological progression in the setting of decreasing tumour marker decline is seen which would necessitate surgical resection prior to the completion of chemotherapy.
- 2010 CUA Guidelines: In most cases, the full course of chemotherapy should be completed and resection of the growing and residual masses should be done post-chemotherapy.
CS IIC and III NSGCT[edit | edit source]
- Induction chemotherapy with cisplatin-based regimens
- Regimen and number of cycles are based on IGCCCG risk classification (see above)
- Good risk NSGCT: BEP×3 or EP×4
- 5-year OS is 91-94%
- Intermediate or poor risk NSGCT: BEP×4
- 5-year OS is 79% for intermediate-risk patients and 48% for poor-risk patients.
- VIP×4 may be substituted for BEP×4 in patients with compromised pulmonary function and in patients in whom extensive chest surgery is likely to be performed to remove residual disease after chemotherapy
- Good risk NSGCT: BEP×3 or EP×4
- Regimen and number of cycles are based on IGCCCG risk classification (see above)
Special scenarios[edit | edit source]
Residual masses after chemotherapy for NSGCT[edit | edit source]
- After receiving first-line cisplatin-based chemotherapy, 5-15% of patients will have partial remission with positive tumour markers or have disease progression.
- Management
- If serum tumour markers elevated after induction chemotherapy, in general patients should receive salvage chemotherapy
- 'If serum tumour markers normal and
- 'Residual mass >1 cm: resection of residual mass
- 'Residual mass <1 cm: controversial management
- If the mass was retroperitoneal, a full bilateral template RPLND should be performed.
- PC-RPLND in NSGCT
- Distribution of histology[14]:
- Necrosis/fibrosis (≈40%)
- Teratoma (≈45%)
- Viable (≈15%) malignancy (with or without teratoma)
- ≈6-8% of post-chemotherapy surgery specimens contain evidence of non-GCT malignancy arising from malignant transformation of teratoma
- While those with necrosis could theoretically avoid post-chemotherapy surgery, necrosis only in the retroperitoneum cannot be predicted with sufficient accuracy to obviate safely the need for post-chemotherapy surgery in patients with residual masses.
- Pure embryonal carcinoma in the primary tumour is the best predictor of fibrosis only in the retroperltoneum
- 90% long-term survival with fibrosis and/or teratoma only at PC-RPLND vs. 50-70% for patients demonstrating viable GCT at PC-RPLND
- If PC-RPLND pathology demonstrates (2021 NCCN TEST-12)
- Teratoma or necrosis/fibrosis: surveillance
- Viable disease (e.g. residual embryonal carcinoma, yolk sac, choriocarcinoma, seminoma) in PC-RPLND pathology: 2 cycles chemotherapy (EP (etoposide/ciplatin), TIP (paclitaxel, ifosfamide, cisplatin), VIP (etoposide, ifosfamide, cisplatin), or VeIP (vinblastine, ifosfamide, cisplatin) [2021 NCCN Guidelines]
- Distribution of histology[14]:
- FDG-PET has NO role in the assessment of patients with NSGCT and residual masses after chemotherapy
- Patients with residual masses at multiple anatomic sites (retroperitoneum, chest, and left supraclavicular fossa are the most common) and normal tumour markers should undergo resection of all sites of measurable residual disease.
- RPLND should be performed before post-chemotherapy surgery at other sites because the probability of residual disease in the retroperitoneum is highest, and RPLND histology is a strong predictor of histology at other sites. Therefore, if no disease in retroperitoneum, unlikely to have any disease elsewhere.
- If RPLND histology shows
- Viable malignancy, then patient should undergo chemotherapy
- Fibrosis, then patient should undergo surveillance or resection
- Teratoma, then patient should undergo resection.
- If RPLND histology shows
- RPLND should be performed before post-chemotherapy surgery at other sites because the probability of residual disease in the retroperitoneum is highest, and RPLND histology is a strong predictor of histology at other sites. Therefore, if no disease in retroperitoneum, unlikely to have any disease elsewhere.
Relapsing NSGCT[edit | edit source]
- Treatment depends on what treatment the patient previously received and, in certain cases, the location of the relapse.
- Chemotherapy-naïve:
- First-line chemotherapy based on ICCCG risk classification
- Cure rates > 95%
- Select CS I patients on surveillance who relapse in the retroperitoneum with non-bulky (<3 cm) tumor and normal serum tumor markers may be treated by induction chemotherapy or RPLND (particularly if teratoma was present in the primary tumor)
- Relapse after chemotherapy:
- Salvage-line chemotherapy.
- Patients with serologic complete response to second-line chemotherapy with residual masses should undergo surgical resection after salvage chemotherapy.
- Patients with viable malignancy in post–salvage chemotherapy surgical specimens have a particularly poor prognosis, and their survival is not improved with the use of postoperative chemotherapy.
- In general, late relapse is resistant to chemotherapy, and the outcome is related to the ability to render patients disease-free by complete surgical resection
Scrotal exploration[edit | edit source]
- Patients found to have NSGCT in orchiectomy pathology following scrotal exploration require further treatment
- Low-stage NSGCT: wide excision of scrotal scar and removal of spermatic cord.
- High-stage NSGCT: systemic therapy will be given and therefore hemiscrotectomy is not needed
[edit | edit source]
- Early toxicity
- Chemotherapy
- Cisplatin is associated with fatigue, myelosuppression, infection, peripheral neuropathy, hearing loss, diminished renal function, and death.
- Etoposide is associated with myelosuppression
- Radiation
- Associated fatigue, nausea and vomiting, leukopenia, and dyspepsia
- Chemotherapy
- Late toxicity
- Hypogonadism
- Occurs in
- 10-20% of patients treated with orchiectomy alone
- 15-40% of patients treated with radiation therapy
- 20-25% of patients treated with first-line chemotherapy regimens
- Serum AM testosterone and luteinizing hormone levels should be measured in patients with signs and symptoms of hypogonadism
- Occurs in
- Infertility
- Most males are able to have biological children after treatment for GCT but paternity rates are lower for men treated with radiation therapy and/or chemotherapy
- Cardiovascular disease
- Risk increased with either subdiaphragmatic radiation or platinum-based chemotherapy
- Patients should establish regular care with a primary care physician so that modifiable risk factors for cardiovascular disease (e.g., diet, exercise, smoking, serum lipid levels, blood pressure, serum glucose) can be monitored.
- Secondary malignancy
- Risk increased with either subdiaphragmatic radiation or platinum-based chemotherapy
- Patients should establish regular care with a primary care physician for appropriate health care maintenance and cancer screening as appropriate.
- Chemotherapy specific
- Bleomycin
- Pulmonary complications (including pulmonary fibrosis)
- Raynaud phenomenon
- Mild myelosuppressive effects at high doses.
- Cisplatin
- Nephrotoxicity
- Neurotoxicity
- Peripheral neuropathy
- Hearing loss
- Bleomycin
- Hypogonadism
Special scenarios[edit | edit source]
Brain metastases[edit | edit source]
- Associated with choriocarcinoma; should be suspected in any patient with a very high serum hCG level
- Choriocarcinomas are highly vascular and tend to hemorrhage during chemotherapy, with death rates of 4-10% secondary to intracranial hemorrhage
- Management
- Brain metastases at diagnosis: BEP×4 chemotherapy followed by resection of residual masses.
- Relapse in the brain after first-line chemotherapy: second-line chemotherapy followed by resection and/or radiation therapy
- Relapse in the brain after achieving a complete response to chemotherapy have a worse prognosis than patients with brain involvement at diagnosis.
Primary extra-gonadal GCTs[edit | edit source]
- Site of origin of GCTs: gonadal (95%) vs. extra-gonadal (5%)
- Develop in midline anatomic locations
- Most common sites (descending order) of origin: mediastinum, retroperitoneum, sacrococcygeal region, and pineal gland, although many unusual sites have also been reported [SASP 2014]
- Primary mediastinal GCT
- NSGCT
- Compared to NSGCTs originating in the testicle or retroperitoneum, primary mediastinal NSGCTs are (4):
- More likely to have yolk sac tumour components and be associated with elevated AFP
- Associated with Klinefelter syndrome
- Less sensitive to chemotherapy
- Associated with a poor prognosis
- Compared to NSGCTs originating in the testicle or retroperitoneum, primary mediastinal NSGCTs are (4):
- Seminoma
- Primary mediastinal seminomas have similar prognosis to testicular seminomas
- NSGCT
- Primary retroperitoneal GCT
- Behave similarly to testicular GCTs and carry the same prognosis.
- Of patients with metastatic GCT without a testis mass:
- 1/3 definitively have a primary extra-gonadal GCT
- 1/3 have ITGCN in the testis
- 1/3 have sonographic evidence of a “burned-out” primary tumor
- Diagnosis and evaluation
- If midline mass in male age < 40, consider GCT
- Midline mass in male age < 40 with elevated AFP and/or hCG is diagnostic of GCT, even if testicular evaluation is normal; histologic confirmation by biopsy is unnecessary before starting treatment
- Midline mass in male age < 40 with normal serum tumor markers, perform biopsy of the midline mass to confirm the diagnosis before beginning treatment
- If midline mass in male age < 40, consider GCT
- Management
- Inguinal orchiectomy
- Indications in patients with suspected extra-gonadal GCT (2):
- Pattern of metastasis is consistent with a right-sided or left-sided testicular primary tumor
- Sonographic evidence of a “burned-out” primary tumor
- Inguinal orchiectomy
Small (<10 mm), impalpable intratesticular lesions[edit | edit source]
- Small (<10 mm), impalpable intratesticular lesions in the absence of disseminated GCT or elevated serum tumor markers are a diagnostic dilemma
- Most of these lesions are benign (testicular cysts, small infarcts, or small Leydig cell or Sertoli cell tumors), however, 20-50% may represent small GCTs (usually seminomas).
- Risk of malignancy increases with the size of the lesion.
- Management options (3):
- Inguinal orchiectomy
- Testis-sparing surgery involving inguinal exploration and excision (with frozen-section analysis to rule out GCT)
- Intraoperative ultrasonography is useful during surgical exploration of the testis to locate the lesion.
- Close observation with serial ultrasound scans (with exploration of growing lesions).
Questions[edit | edit source]
- Which subtypes comprise non-seminoma germ-cell tumours?
- What percentage of patients are found to have metastatic disease at the time of diagnosis?
- Which tumours secrete AFP? hCG? What is the half-life of these tumour markers?
- What is the primary landing zone of a left vs. right primary testicular tumour?
- What is the management of a post-chemotherapy retroperitoneal mass?
Answers[edit | edit source]
- Which subtypes comprise non-seminoma germ-cell tumours?
- What percentage of patients are found to have metastatic disease at the time of diagnosis?
- Which tumours secrete AFP? hCG? What is the half-life of these tumour markers?
- What is the primary landing zone of a left vs. right primary testicular tumour?
- What is the management of a post-chemotherapy retroperitoneal mass?
References[edit | edit source]
- Wein AJ, Kavoussi LR, Partin AW, Peters CA (eds): CAMPBELL-WALSH UROLOGY, ed 11. Philadelphia, Elsevier, 2015, chap 34
- Stephenson, Andrew, et al. "Diagnosis and treatment of early stage testicular cancer: AUA guideline." The Journal of urology 202.2 (2019): 272-281.
- Wood, Lori, et al."Canadian consensus guidelines for the management of testicular germ cell cancer." Canadian Urological Association Journal 4.2 (2010): e19.