Incontinence after Prostate Therapy (2024): Difference between revisions
Jump to navigation
Jump to search
Urology4all (talk | contribs) |
Urology4all (talk | contribs) No edit summary |
||
| (11 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
* '''See [https://pubmed.ncbi.nlm.nih.gov/38934789/ Original Guidelines]''' | * '''See [https://pubmed.ncbi.nlm.nih.gov/38934789/ Original Guidelines]''' | ||
** '''See [https://www.auanet.org/documents/Guidelines/IPT%20EVALUATION%20ALGORITHM.png Evaluation Algorithm]''' | |||
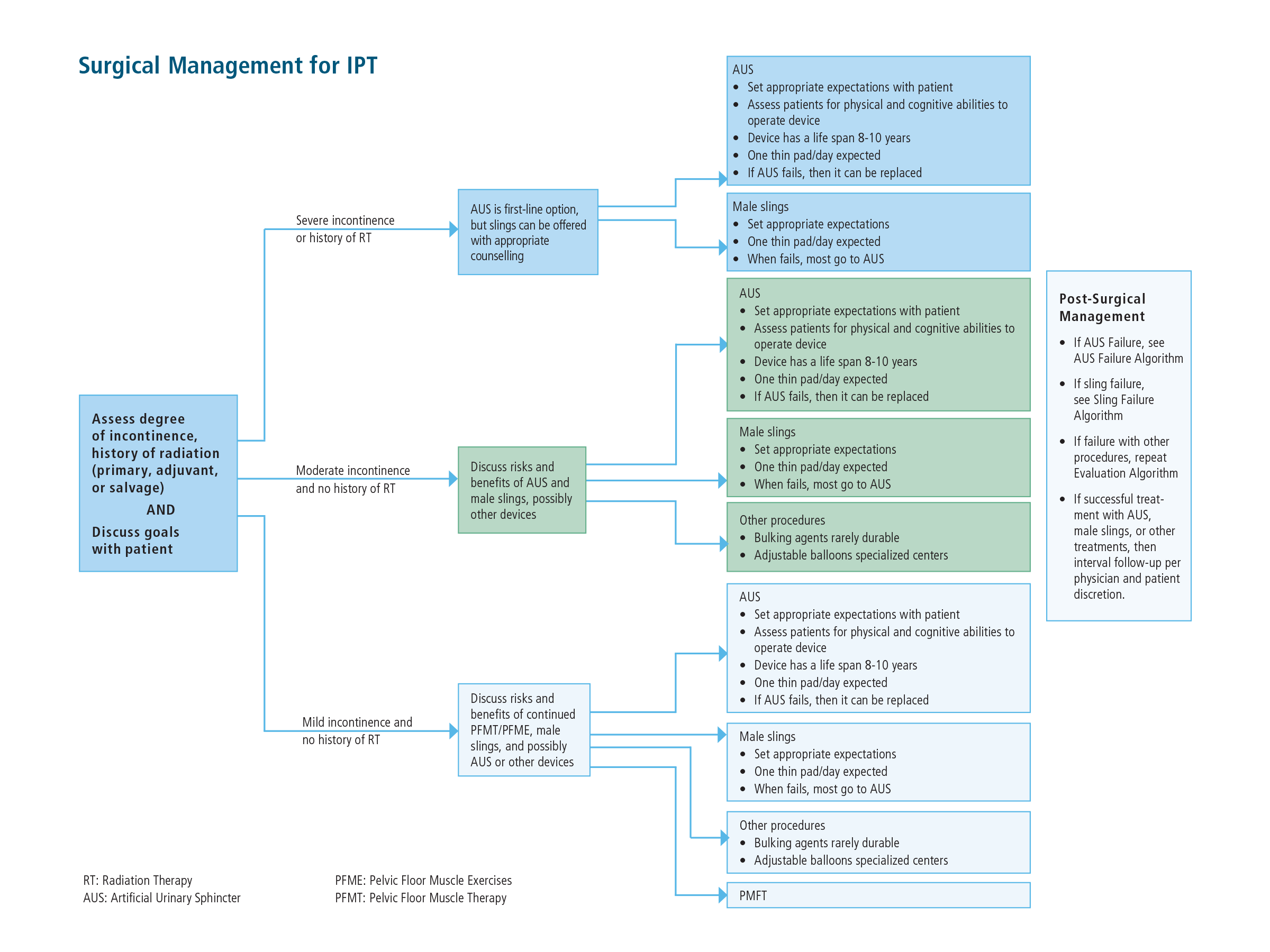
** '''See [https://www.auanet.org/documents/Guidelines/IPT%20SURGICAL%20MANAGEMENT%20ALGORITHM.png Surgical Management Algorithm]''' | |||
** '''See [https://www.auanet.org/documents/Guidelines/IPT%20SLING%20FAILURE%20ALGORITHM.png Sling Failure Algorithm]''' | |||
** '''See [https://www.auanet.org/documents/Guidelines/PDF/2024%20Guidelines/AUS%20Failure%20Algorithm.pdf AUS Failure Algorithm]''' | |||
* '''See [[Functional: Surgery for Male SUI|Male SUI Surgery]] Chapter Notes''' | * '''See [[Functional: Surgery for Male SUI|Male SUI Surgery]] Chapter Notes''' | ||
| Line 127: | Line 131: | ||
*Conservations options may be utilized while engaging in PFME/PFMT, considering future options, waiting an appropriate time before surgical intervention, or as an indefinite form of management. | *Conservations options may be utilized while engaging in PFME/PFMT, considering future options, waiting an appropriate time before surgical intervention, or as an indefinite form of management. | ||
==== | ==== PFME/PFMT ==== | ||
* '''<span style="color:#ff0000">Should be offered to all patients seeking treatment for incontinence after RP</span>''' | * '''<span style="color:#ff0000">Should be offered to all patients seeking treatment for incontinence after RP</span>''' | ||
* Advantages: | * Advantages: | ||
| Line 137: | Line 141: | ||
* '''<span style="color:#ff0000">Other non-surgical options can be used with or without PFME/PFMT</span>''' | * '''<span style="color:#ff0000">Other non-surgical options can be used with or without PFME/PFMT</span>''' | ||
==== | ==== Absorbent pads (Liners, Guards, Briefs, Underwear) ==== | ||
* Primary tool of urinary containment. | * Primary tool of urinary containment. | ||
* In general, milder incontinence is managed satisfactorily with shields or lower density guards, while severe incontinence requires briefs or underwear with or without inserts to prevent accidents. | * In general, milder incontinence is managed satisfactorily with shields or lower density guards, while severe incontinence requires briefs or underwear with or without inserts to prevent accidents. | ||
| Line 143: | Line 147: | ||
* Use of pads may be associated with skin irritation and dermatitis | * Use of pads may be associated with skin irritation and dermatitis | ||
==== | ==== Penile compression devices (clamps) ==== | ||
* Can be used independently and as an adjunct to reduce daily absorbent product usage. | * Can be used independently and as an adjunct to reduce daily absorbent product usage. | ||
* Patients must be instructed to release the clamp every | * '''Patients must be instructed to release the clamp every 2 hours to allow for circulation regardless of the need to void. The clamp should not be left on the phallus overnight due to the risks of constant pressure.''' | ||
* <span style="color:#ff0000">'''Not suitable for patients with (4):'''</span> | * <span style="color:#ff0000">'''Not suitable for patients with (4):'''</span> | ||
*# <span style="color:#ff0000">'''Memory deficits'''</span> | *# <span style="color:#ff0000">'''Memory deficits'''</span> | ||
| Line 152: | Line 156: | ||
*# <span style="color:#ff0000">'''Significant component of OAB'''</span> | *# <span style="color:#ff0000">'''Significant component of OAB'''</span> | ||
==== | ==== Catheters ==== | ||
* May be necessary in patients with high volume pad usage suffering from skin excoriation, dermatitis, and cellulitis due to urinary leakage. | * '''May be necessary in patients with high volume pad usage suffering from skin excoriation, dermatitis, and cellulitis due to urinary leakage.''' | ||
* Also advantageous when the number or frequency of absorbent product changes is disruptive and/or financially prohibitive. | * Also advantageous when the number or frequency of absorbent product changes is disruptive and/or financially prohibitive. | ||
===== | ===== Condom catheter ===== | ||
* Effective method of urinary containment for men with severe incontinence. | * Effective method of urinary containment for men with severe incontinence. | ||
* In comparison to compressive devices, condom catheter systems are acceptable for patients with any degree of urge incontinence. Theoretically, this approach would also be superior to urethral catheterization due to the avoidance of mechanical bladder irritation. | * In comparison to compressive devices, condom catheter systems are acceptable for patients with any degree of urge incontinence. Theoretically, this approach would also be superior to urethral catheterization due to the avoidance of mechanical bladder irritation. | ||
* Unsuitable for patients with | * '''Unsuitable for patients with''' | ||
* | *# '''A retractile phallus''' | ||
* | *# '''Skin excoriation''' | ||
* | *# '''Concomitant urethral stricture''' | ||
* | *# '''Poor manual dexterity''' | ||
* | *# '''A large glans/narrow phallus configuration''' | ||
*The condom or sheath varies based on the material (latex or silicone), length of adhesive surface, circumference, and overall length | *The condom or sheath varies based on the material (latex or silicone), length of adhesive surface, circumference, and overall length | ||
*Success of a condom catheter is wholly dependent on proper sizing. | *'''Success of a condom catheter is wholly dependent on proper sizing.''' | ||
===== | ===== Urethral catheter ===== | ||
* '''<span style="color:#ff0000">Last resort</span>''' in a patient who is unsuitable for alternative management | * '''<span style="color:#ff0000">Last resort</span>''' in a patient who is unsuitable for alternative management | ||
* '''Suprapubic catheter drainage is not a solution for the patient with severe intrinsic sphincter deficiency, as urethral leakage will persist''' | * '''Suprapubic catheter drainage is not a solution for the patient with severe intrinsic sphincter deficiency, as urethral leakage will persist''' | ||
| Line 175: | Line 179: | ||
==== Timing ==== | ==== Timing ==== | ||
* '''<span style="color:#ff0000">In patients with bothersome stress urinary incontinence after prostate treatment, clinicians | * '''<span style="color:#ff0000">In patients with bothersome stress urinary incontinence after prostate treatment despite conservative therapy, clinicians</span>''' | ||
** Patients who report a lack of symptom improvement or those experiencing more severe incontinence at | ** '''<span style="color:#ff0000">May offer surgery as early as 6 months if incontinence</span>''' | ||
*'''<span style="color:#ff0000"> | *** Patients who report a lack of symptom improvement or those experiencing more severe incontinence at 6months may be offered early treatment in the form of surgical interventions with such a treatment decision made using a shared decision-making model. | ||
**'''<span style="color:#ff0000">Majority of patients will reach their maximum improvement by 12 months with minimal to no improvement afterwards.</span>''' | **'''<span style="color:#ff0000">Should offer surgical treatment at 12 months post-prostate treatment.</span>''' | ||
*** Withholding surgical treatment after 12 months is unlikely to result in improved patient symptoms and will delay restoration of continence. | ***'''<span style="color:#ff0000">Majority of patients will reach their maximum improvement by 12 months with minimal to no improvement afterwards.</span>''' | ||
* | **** Withholding surgical treatment after 12 months is unlikely to result in improved patient symptoms and will delay restoration of continence. | ||
*** Conversely, treatment should be offered with caution in patients who are displaying symptom improvement. | **** Conversely, treatment should be offered with caution in patients who are displaying symptom improvement. | ||
==== Pre-surgical Evaluation ==== | ==== Pre-surgical Evaluation ==== | ||
| Line 187: | Line 191: | ||
#* '''Demonstrate SUI on physical exam''', with or without provocative testing such as bending, shifting position, or rising from seated to standing position | #* '''Demonstrate SUI on physical exam''', with or without provocative testing such as bending, shifting position, or rising from seated to standing position | ||
#* Stress pad testing can also be performed. | #* Stress pad testing can also be performed. | ||
#* If there is any doubt as to whether the patient has SUI, UDS may be performed | #* If there is any doubt as to whether the patient has SUI, UDS may be performed. | ||
# '''<span style="color:#ff0000">Cystourethroscopy should be performed to assess for urethral and bladder pathology that may affect outcomes of surgery</span>''' | # '''<span style="color:#ff0000">Cystourethroscopy should be performed to assess for urethral and bladder pathology that may affect outcomes of surgery</span>''' | ||
#* '''The presence of urethral pathology (e.g., stricture, BNC, urethral lesions) may affect the outcome of surgery''' | #* '''The presence of urethral pathology (e.g., stricture, vesicourethral anastomotic stenosis (VUAS), BNC, urethral lesions) may affect the outcome of surgery''' | ||
#* Cystourethroscopy has also been recommended prior to placement of transobturator slings to assess urethral function (patients should have visual voluntary contraction of the external sphincter), and luminal closure of the urethra should be demonstrated with bulbar compression and elevation (repositioning test). However, success of the procedure has not been shown to be dependent on these findings in any controlled study. | #** Cystourethroscopy has also been recommended prior to placement of transobturator slings to assess urethral function (patients should have visual voluntary contraction of the external sphincter), and luminal closure of the urethra should be demonstrated with bulbar compression and elevation (repositioning test). However, success of the procedure has not been shown to be dependent on these findings in any controlled study. | ||
#*''' | #**'''Patients with symptomatic VUAS or BNC should be treated prior to surgery for IPT''' | ||
#*In cases where pre-operative cystourethroscopy is not performed, it may be done at the start of the AUS or sling implantation before any incision is made. In such cases, patients should be made aware of the potential consequences and the possibility of aborting an AUS or sling insertion if significant urethral or bladder pathology is discovered. | #***Although a VUAS or BNC will not necessarily cause SUI, treatment of them may worsen SUI. This is important because a patient may be considered for a sling procedure if he had “mild” incontinence, but he would likely need an AUS if it worsens after treatment. | ||
#***'''Following treatment of VUAS, an interval cystoscopy should be performed at least 4-6 weeks later to document improvement and stabilization, after which IPT treatment can be considered.''' | |||
#*In cases where pre-operative cystourethroscopy is not performed, it may be done at the start of the AUS or sling implantation before any incision is made. | |||
#**In such cases, patients should be made aware of the potential consequences and the possibility of aborting an AUS or sling insertion if significant urethral or bladder pathology is discovered. | |||
# '''<span style="color:#ff0000">Urodynamics (UDS) may be performed in cases where it may facilitate diagnosis or counseling.</span>''' | # '''<span style="color:#ff0000">Urodynamics (UDS) may be performed in cases where it may facilitate diagnosis or counseling.</span>''' | ||
#* Can aid in determining if IPT is cause by sphincter dysfunction, bladder dysfunction, or a combination of both, and also assess bladder contractility and the presence of bladder outlet dysfunction. | #* Can aid in determining if IPT is cause by sphincter dysfunction, bladder dysfunction, or a combination of both, and also assess bladder contractility and the presence of bladder outlet dysfunction. | ||
| Line 202: | Line 207: | ||
#** Similarly, detrusor over-activity found on UDS has not been shown to negatively impact sling outcomes in men with SUI after prostate treatment. | #** Similarly, detrusor over-activity found on UDS has not been shown to negatively impact sling outcomes in men with SUI after prostate treatment. | ||
#** Abdominal leak-point pressure has not been shown to affect outcomes of AUS | #** Abdominal leak-point pressure has not been shown to affect outcomes of AUS | ||
#** if the clinician is unsure of how prevalent sphincteric versus bladder affecting incontinence, or if there is unexplained poor bladder emptying, then UDS may be helpful in providing that additional information. | #** if the clinician is unsure of how prevalent sphincteric versus bladder affecting incontinence, or if there is unexplained poor bladder emptying, then UDS may be helpful in providing that additional information. Examples of this may be | ||
#* ''' | #*** Patient reports significant mixed incontinence and stress incontinence is not demonstrated | ||
#*** Impaired compliance is suspected and incontinence could be related to high storage pressures without urgency | |||
#*** Overflow incontinence is suspected (PVR) may be helpful to rule out significant retention of urine) | |||
#* '''<span style="color:#ff0000">★In patients with suspected SUI who do not demonstrate SUI during UDS with a catheter in place, it is important that the catheter be removed and stress testing repeated''' | |||
#** Up to 35% of males with post-prostatectomy SUI will not demonstrate SUI with a catheter in place. This may be due to some scarring at the site of the anastomosis. In such cases, even a small catheter can occlude the urethra and prevent stress leakage. | #** Up to 35% of males with post-prostatectomy SUI will not demonstrate SUI with a catheter in place. This may be due to some scarring at the site of the anastomosis. In such cases, even a small catheter can occlude the urethra and prevent stress leakage. | ||
| Line 217: | Line 225: | ||
# '''<span style="color:#ff0000">Urinary Diversion</span>''' | # '''<span style="color:#ff0000">Urinary Diversion</span>''' | ||
===== Urethral bulking agents ===== | ===== Urethral bulking agents ===== | ||
* | * '''Most commonly used procedure to treat male SUI''' | ||
* Considered off-label | |||
** Currently no FDA-approved available agents for the treatment of male incontinence | ** Currently no FDA-approved available agents for the treatment of male incontinence | ||
| Line 244: | Line 253: | ||
**Most common intraoperative complication is urethral or bladder perforation | **Most common intraoperative complication is urethral or bladder perforation | ||
**Mean all-cause (i.e., erosion, infection, balloon migration or balloon failure) explantation rate is 27%, more common that AUS | **Mean all-cause (i.e., erosion, infection, balloon migration or balloon failure) explantation rate is 27%, more common that AUS | ||
**Efficacy, complication rates, and complication types have been associated with volume. | **Efficacy, complication rates, and complication types have been associated with surgeon volume. | ||
***Obtaining specialty training from an experienced implanter would be beneficial before device implantation. | ***Obtaining specialty training from an experienced implanter would be beneficial before device implantation. | ||
| Line 261: | Line 270: | ||
**'''<span style="color:#ff0000">Poor efficacy in comparison to an AUS</span>''' | **'''<span style="color:#ff0000">Poor efficacy in comparison to an AUS</span>''' | ||
====== | ====== Complications ====== | ||
* Generally low complication rate | * Generally low complication rate | ||
* '''Urinary retention''' | * '''Urinary retention''' | ||
| Line 277: | Line 286: | ||
*#* Patients with IPT following primary, adjuvant or salvage RT should be offered the same conservative management as a patient with postprostatectomy SUI. Patients who fail conservative measures should be offered surgical management, preferably placement of AUS. | *#* Patients with IPT following primary, adjuvant or salvage RT should be offered the same conservative management as a patient with postprostatectomy SUI. Patients who fail conservative measures should be offered surgical management, preferably placement of AUS. | ||
*#* Radiated patients undergoing AUS placement should be counseled on potentially compromised functional outcomes and an increased risk of complications. | *#* Radiated patients undergoing AUS placement should be counseled on potentially compromised functional outcomes and an increased risk of complications. | ||
*#* '''Slings may be a potential option in some radiated patients but adjustable balloons are significantly less effective''' | *#* '''Slings may be a potential option in some radiated patients but adjustable balloons are significantly less effective [different than 2019 guidelines which only supported AUS after radiation]''' | ||
*# '''<span style="color:#ff0000">Urethral reconstruction</span>''' | *# '''<span style="color:#ff0000">Urethral reconstruction</span>''' | ||
*#* Urethral strictures of the anterior urethra and urethral stenosis of the posterior urethra can arise after RP, RT, or treatment for IPT. Urethral reconstructive surgery is often used to treat narrowing in the urethra. | *#* Urethral strictures of the anterior urethra and urethral stenosis of the posterior urethra can arise after RP, RT, or treatment for IPT. Urethral reconstructive surgery is often used to treat narrowing in the urethra. | ||
*#* '''Male slings will not be effective given post-surgical changes related to most types of urethral reconstruction in the posterior and anterior urethra''' | *#* '''Male slings will not be effective given post-surgical changes related to most types of urethral reconstruction in the posterior and anterior urethra''' | ||
*#* '''Complications rates are higher''' | *#* '''Complications rates are higher''' | ||
*#** Depending on the technique employed (urethra transecting or not) the blood supply to the urethra may be diminished and potentially decrease the life span of an AUS. | *#** Depending on the technique employed (urethra transecting or not) the blood supply to the urethra may be diminished and potentially decrease the life span of an AUS. | ||
| Line 300: | Line 309: | ||
** '''<span style="color:#ff0000">If identified during implantation, procedure should be abandoned and subsequent implantation should be delayed</span>''' | ** '''<span style="color:#ff0000">If identified during implantation, procedure should be abandoned and subsequent implantation should be delayed</span>''' | ||
* '''<span style="color:#ff0000">Persistent leakage</span>''' | * '''<span style="color:#ff0000">Persistent leakage</span>''' | ||
* '''<span style="color:#ff0000"> | * '''<span style="color:#ff0000">Erosion</span>''' | ||
* '''<span style="color:#ff0000">Infection</span>''' | * '''<span style="color:#ff0000">Infection</span>''' | ||
* '''<span style="color:#ff0000">Mechanical failure</span>''' | * '''<span style="color:#ff0000">Mechanical failure</span>''' | ||
*'''<span style="color:#ff0000">Decreased efficacy over time and reoperations are common</span>''' | *'''<span style="color:#ff0000">Decreased efficacy over time and reoperations are common</span>''' | ||
** '''The current version consists of''' a hydraulic system composed of '''3 separate parts:''' | ** '''The current version consists of''' a hydraulic system composed of '''3 separate parts:''' | ||
| Line 341: | Line 327: | ||
**A malfunctioning AUS does not necessarily need to be replaced, but if the patient is healthy and requests a replacement, the AUS can be explanted and a new one replaced at the same operative setting. | **A malfunctioning AUS does not necessarily need to be replaced, but if the patient is healthy and requests a replacement, the AUS can be explanted and a new one replaced at the same operative setting. | ||
***The durability and efficacy of a secondary re-implant in this setting is the same as that of a primary AUS, except in the setting of erosion | ***The durability and efficacy of a secondary re-implant in this setting is the same as that of a primary AUS, except in the setting of erosion | ||
*Risk factors for complications | |||
** Radiation | |||
** Urethral compromise | |||
*** Can be due to surgical intervention, including urethroplasty, multiple treatments for BNC or stricture, urethral stent placement, and prior AUS erosion1 | |||
===== Urinary diversion ===== | ===== Urinary diversion ===== | ||
| Line 371: | Line 361: | ||
# '''<span style="color:#ff0000">Wear or urethral atrophy</span>''' | # '''<span style="color:#ff0000">Wear or urethral atrophy</span>''' | ||
#*'''Recurrent incontinence after years of normal function suggests either development of a new leak due to wear or urethral atrophy''' | #*'''Recurrent incontinence after years of normal function suggests either development of a new leak due to wear or urethral atrophy''' | ||
#**Cystoscopy is the mainstay for evaluation of atrophy and erosion. | |||
#**A leak can be confirmed by decreased volume in the pressure regulating balloon, which can be assessed by using ultrasound or computerized tomography. | #**A leak can be confirmed by decreased volume in the pressure regulating balloon, which can be assessed by using ultrasound or computerized tomography. | ||
# '''<span style="color:#ff0000">Elevated storage pressures or detrusor over-activity</span>''' | # '''<span style="color:#ff0000">Elevated storage pressures or detrusor over-activity</span>''' | ||
#*'''Should be suspected in a patient with a normally functioning AUS''' | #*'''Should be suspected in a patient with a normally functioning AUS''' | ||
| Line 392: | Line 382: | ||
=== Patients presenting with infection or erosion of AUS or sling === | === Patients presenting with infection or erosion of AUS or sling === | ||
* | *'''<span style="color:#ff0000">Erosion</span>''' | ||
** Timing of removal is usually influenced by severity of the infection and acuity of the clinical situation as indicated by the associated signs and symptoms (e.g., purulent drainage, erythema, tenderness, fever, chills). | **'''A devastating complication that can lead to urine extravasation, infection, abscess formation and sepsis, and may result in long-term urethral fistula, urethral diverticula, or urethral stricture after AUS explant.''' | ||
* In the case of the AUS, the most conservative course of action is removal of all components, regardless of whether the infection and any associated reaction are limited to a single component. | ** Incidence | ||
* An infected male sling should be removed as completely as feasible without damaging any adjacent structures. | *** Occurs in 1-10% of cases on long-term follow-up | ||
* | ** Pathophysiology | ||
*** Can be due to unrecognized urethral injury at the time of initial surgery or more likely due to subsequent instrumentation of the urethra including catheterization. | |||
** '''Diagnosis and Evaluation''' | |||
*** '''Generally presents with with hematuria, dysuria, or difficulty emptying the bladder and is diagnosed with a cystoscopic demonstration of the AUS cuff within the urethra''' | |||
** '''<span style="color:#ff0000">Management:''' | |||
*** '''<span style="color:#ff0000">Explanting eroded device with urethral catheter alone, in situ urethroplasty, or anastomotic urethroplasty''' | |||
**** During explant, the goal of erosion management is to maximize the chances of urethral healing without developing a fistula or stricture. | |||
**** The degree of urethral loss with erosion can be highly variable, ranging from a small <5mm hole in the urethra, to complete circumferential urethral loss under the 2cm cuff. | |||
***** '''<span style="color:#ff0000">The urethral defect will usually heal by leaving a urethral catheter in place for 3 weeks.''' | |||
***** Some authors, however, recommend a urethral repair in cases of larger urethral defects due to decreased rates of stricture. The decision on how to best manage the erosion takes into consideration the size of the urethral defect, quality of local tissues (there are heterogeneous degrees of inflammation, induration, and fibrosis), and surgeon preference/experience. | |||
* '''<span style="color:#ff0000">Infection</span>''' | |||
** Often times an infection is secondary to a pre-existing erosion. | |||
*** AUS isolated cuff infections are rare without an associated erosion. | |||
** '''<span style="color:#ff0000">Incidence''' | |||
*** '''<span style="color:#ff0000">Device infection occurs in <1-5% of cases''' | |||
** '''<span style="color:#ff0000">Diagnosis and Evaluation''' | |||
***'''<span style="color:#ff0000">History and Physical Exam''' | |||
****'''<span style="color:#ff0000">Presents with (4):''' | |||
****#'''<span style="color:#ff0000">Pain at the site of the AUS''' | |||
****#'''<span style="color:#ff0000">Fever''' | |||
****#'''<span style="color:#ff0000">Scrotal warmth or erythema''' | |||
****#'''<span style="color:#ff0000">Skin changes''' | |||
** '''<span style="color:#ff0000">Management:''' | |||
*** '''<span style="color:#ff0000">Explantation should be performed as soon as possible''' | |||
**** '''Timing of removal is usually influenced by severity of the infection and acuity of the clinical situation as indicated by the associated signs and symptoms (e.g., purulent drainage, erythema, tenderness, fever, chills).''' | |||
**** '''In the case of the AUS, the most conservative course of action is removal of all components, regardless of whether the infection and any associated reaction are limited to a single component.''' | |||
**** '''An infected male sling should be removed as completely as feasible without damaging any adjacent structures.''' | |||
* '''<span style="color:#ff0000">For patients seeking a replacement device (AUS or male sling) after infection and/or erosion, a waiting period of 3-6 months is recommended.''' | |||
** '''In the AUS patient, it may be necessary to proceed with transcorporal placement of the cuff to place the cuff at a different location along the urethra.''' | |||
=== Sexual arousal incontinence or climacturia === | === Sexual arousal incontinence or climacturia === | ||
| Line 414: | Line 429: | ||
*** Rate of device infection, erosion or malfunction was not increased in combined compared to staged procedures. | *** Rate of device infection, erosion or malfunction was not increased in combined compared to staged procedures. | ||
*** Similar continence, sexual function, and overall satisfaction in patients undergoing staged versus combined procedures | *** Similar continence, sexual function, and overall satisfaction in patients undergoing staged versus combined procedures | ||
== Questions == | == Questions == | ||
Latest revision as of 11:37, 28 July 2025
- See Original Guidelines
- See Male SUI Surgery Chapter Notes
{kind=link}
{kind=link}
{kind=link}
Background[edit | edit source]
- Commonly accepted definition of urinary continence: not requiring a pad or protective device to stay dry (pad-free)
- Social continence: ≤1 pad per day that is tolerable to the patient.
- Severity of continence
- Mild: 1-2 pads per day
- Moderate: 2-4 pads per day
- Severe: >5 pads per day
- Incontinence after prostate therapy (IPT) is caused by damage to the striated muscle and nerve fibers of the voluntary (striated) urethral sphincter
- The term “incontinence after prostate treatment” is used in this guideline over the familiar term “post-prostatectomy incontinence” because it is more inclusive and covers males who have incontinence after undergoing radical prostatectomy (RP), radiotherapy (RT) or BPH-surgery
Pre-treatment Counselling[edit | edit source]
Urinary Incontinence[edit | edit source]
- Inform patients undergoing RP that (2):
- Incontinence is expected in the short-term and generally improves to near baseline by 12 months after surgery but may persist and require treatment
- Most males undergoing RP are not continent (pad-free) at the time of catheter removal and should be informed that continence is not immediate.
- Majority of patients will reach their maximum improvement by 12 months with minimal to no improvement afterwards.
- 90% of patients will achieve continence at 6 months after robotic-assisted laparoscopic prostatectomy and only an additional 4% of patients will gain continence afterwards.
- Conservative management with regular follow-up during the first year after surgery is recommended to assess patient progress
- All known factors that could affect continence (5):
- Older age
- Larger prostate size
- Shorter membranous urethral length (measured by MRI)
- Lack of preservation of bilateral neurovascular bundle at time of RP
- No surgical maneuvers, other than preservation of bilateral neurovascular bundle, results in improved continence recovery at 12 months
- Patients receiving bilateral neurovascular bundle preservation were 26% more likely to be continent at 6 months compared to patients who did not
- Retzius sparing RP may be associated with early return to continence by continence rates at 12 months are similar to other techniques
- Patients with poor pre-operative potency still benefit from nerve sparing in terms of recovery of continence
- No surgical maneuvers, other than preservation of bilateral neurovascular bundle, results in improved continence recovery at 12 months
- Prior pelvic radiation
- Radiation is a significant risk factor for IPT in patients undergoing RP or TURP.
- Radiation causes small vessel obliteration and endarteritis, resulting in ischemic tissue changes such as fibrosis and necrosis
- Urethral fibrosis decreases the functional capabilities of the external sphincter, ultimately affecting continence and outcomes following AUS or sling placement.
- Even in the absence of direct damage to the sphincter, adjacent surgical cautery or laser energy further compromises sphincter function.
- TURP following brachytherapy or external beam radiation has been associated with incontinence rates of up to 70%.
- The need for subsequent resections, patient age, and pre-TURP urgency is correlated with higher rates of incontinence.
- Little to no published evidence discussing post-TURP outcomes with patients who have undergone other forms of local therapy such as HIFU and cryotherapy. However, it is the opinion of this Panel that these patients have high risks of incontinence similar to post-TURP radiated patients.
- Salvage RP, regardless of the initial form of non-operative therapy or the operative approach (open or robotic), is associated with high rates of urinary incontinence rates (20%-70%)
- These patients should be informed that they may require an artificial urinary sphincter (AUS).
- Radiation is a significant risk factor for IPT in patients undergoing RP or TURP.
- Surgical approach: open RP has similar rates of urinary incontinence as robot-assisted RP
- BMI may impact IPT in the short-term; however, not considered to impact risk at 1-year after RP
- Incontinence is expected in the short-term and generally improves to near baseline by 12 months after surgery but may persist and require treatment
Sexual Arousal Incontinence and Climacturia[edit | edit source]
- Inform patients undergoing localized prostate cancer treatment on the risks of sexual arousal incontinence and climacturia
- Sexual arousal incontinence: inadvertent loss of urine during sexual arousal, foreplay, and/or masturbation.
- Climacturia (also known as orgasm associated urinary incontinence): involuntary loss of urine at the time of orgasm.
- Pathophysiology of climacturia is not completely understood.
- The mechanism is thought to relate to removal of the internal sphincter during RP, which is exacerbated by prior transurethral resection of the prostate (TURP). Bladder contraction at the time of orgasms with some degree of external sphincter insufficiency is thought to result in leakage during orgasm.
- Pathophysiology of climacturia is not completely understood.
- Can occur following RP, with or without adjuvant RT, and can even occur following RT alone.
- Occurs in 30% of cases following prostate cancer surgery, 4% after RT
- Ejaculatory dysfunction, such as an anejaculation, is common after radiation
- Occurs in 30% of cases following prostate cancer surgery, 4% after RT
- Risk factors
- Time since surgery (main risk factor; shorter time from surgery is associated with a higher rate of leakage)
- Prior TURP
- Shorter functional urethral and penile length following RP
- Not risk factors: age, pre-operative erectile function, or nerve sparing status
- Improvement can be expected throughout the postoperative period, but it can take several years to resolve, and typically persists in one-third of patients.
Pelvic floor muscle exercises (PFME) or pelvic floor muscle training (PFMT)[edit | edit source]
- Pelvic floor muscle exercise (PFME): an exercise program specific to the pelvic floor muscle group that is self-guided as a home exercise program only.
- The patient may have learned the program through patient education literature or with a single basic instruction session from an appropriate practitioner.
- Pelvic floor muscle training (PFMT): a training program specific to the pelvic floor muscle group that is practitioner guided.
- May be offered prior to RP
- Exercises for the pelvic floor muscle are easier to learn in the pre-operative period since mastery can be difficult postoperatively given muscle inhibition, sensory changes, urinary incontinence, and surgical pain.
- Typical preliminary goals of a preoperative program include proper patient education regarding pelvic floor muscle anatomy, physiology, awareness, and motor control, which maximize the effectiveness of exercises.
- To allow for neuromuscular adaptation, preoperative PFMT should be started three to four weeks prior to surgery.
- The benefit of starting pre-operative PFMT in not consistent in the outcome data.
- Should be offered to all patients after RP upon removal of the urethral catheter
- Improves time to continence (thus improving QoL) but not overall continence at 12 months
- PFME after catheter removal has been shown to improve time-to-achieving continence compared to control groups in RCTs
- Improves time to continence (thus improving QoL) but not overall continence at 12 months
Diagnosis and Evaluation[edit | edit source]
UrologySchool.com Summary[edit | edit source]
- Recommended
- History and Physical Exam
- Other
- Appropriate diagnostic modalities to categorize type and severity of incontinence and degree of bother
- Optional
- Post-void residual
Recommended[edit | edit source]
- History and Physical Exam
- History
- Characterize incontinence (4):
- Type of incontinence (stress, urgency, mixed)
- Treatment for SUI (caused by sphincteric insufficiency) vs. urgency incontinence (caused by bladder dysfunction) are different.
- Increases in abdominal pressure such as that caused by straining, walking, cough, and exercise are suggestive of SUI
- The sudden compelling desire to void that is difficult to defer and results in leakage indicates urgency incontinence.
- Occurrence of urinary frequency, urgency, and urgency urinary incontinence is common after prostate treatment.
- Presence of urgency urinary incontinence should not exclude a patient from surgical treatment of his bothersome SUI.
- In cases of mixed incontinence, determine which component is more prevalent and bothersome (stress or activity related versus urgency related)
- Presence of incontinence while asleep as well as nocturia are also important to note, because this may indicate urgency urinary incontinence or severe SUI.
- Treatment for SUI (caused by sphincteric insufficiency) vs. urgency incontinence (caused by bladder dysfunction) are different.
- Progression or resolution of incontinence over time, exacerbating factors
- Severity of incontinence (i.e. volume lost over time)
- Can be determined by history, or more objectively, by pad testing
- Guide treatment; some surgical treatments (e.g., male slings), clearly have inferior results in severe incontinence.
- Degree of bother
- Type of incontinence (stress, urgency, mixed)
- Status of prostate cancer
- Particularly for candidates for salvage RT, which may impact efficacy of continence treatment.
- Characterize incontinence (4):
- History
Optional[edit | edit source]
- Post-void residual (PVR)
- May be helpful to rule out significant retention of urine if overflow incontinence is suspected.
- A single low PVR value does not rule out the presence of incomplete emptying.
- Threshold value of a significant PVR is similarly undefined.
- Elevated PVR may be an indication of detrusor underactivity or obstruction (e.g., urethral stricture or bladder neck contracture [BNC]) and thus may prompt further diagnostic evaluation such as uroflowmetry, cystoscopy, or multichannel UDS.
- May be helpful to rule out significant retention of urine if overflow incontinence is suspected.
Management[edit | edit source]
- Patients with urgency urinary incontinence or urgency predominant mixed urinary incontinence should be offered treatment options per the AUA Overactive Bladder Guidelines
- Manage patients with SUI after treatment of BPH the same as patients that have undergone RP
- Rate of persistent SUI in patients undergoing open laparoscopic or endoscopic surgical management of BPH ranges between 0% - 8.4%.
- Evaluation of patients with SUI after surgical therapy for BPH should be similar to those who have undergone RP; care must be taken to rule out a primary bladder pathology such as OAB.
Non-surgical[edit | edit source]
Options (5)[edit | edit source]
- PFME/PFMT
- Absorbent pads
- Penile compression devices
- Condom catheter
- Urethral catheter
- Conservations options may be utilized while engaging in PFME/PFMT, considering future options, waiting an appropriate time before surgical intervention, or as an indefinite form of management.
PFME/PFMT[edit | edit source]
- Should be offered to all patients seeking treatment for incontinence after RP
- Advantages:
- Safe treatment with minimal side-effects
- Provides patients with an opportunity to participate in their health outcomes.
- Disadvantages:
- Time and effort required
- Cost of repeated visits for PFMT
- Other non-surgical options can be used with or without PFME/PFMT
Absorbent pads (Liners, Guards, Briefs, Underwear)[edit | edit source]
- Primary tool of urinary containment.
- In general, milder incontinence is managed satisfactorily with shields or lower density guards, while severe incontinence requires briefs or underwear with or without inserts to prevent accidents.
- From a cost perspective, briefs and underwear systems have been demonstrated to be more effective than pads.
- Use of pads may be associated with skin irritation and dermatitis
Penile compression devices (clamps)[edit | edit source]
- Can be used independently and as an adjunct to reduce daily absorbent product usage.
- Patients must be instructed to release the clamp every 2 hours to allow for circulation regardless of the need to void. The clamp should not be left on the phallus overnight due to the risks of constant pressure.
- Not suitable for patients with (4):
- Memory deficits
- Poor manual dexterity
- Impaired sensation
- Significant component of OAB
Catheters[edit | edit source]
- May be necessary in patients with high volume pad usage suffering from skin excoriation, dermatitis, and cellulitis due to urinary leakage.
- Also advantageous when the number or frequency of absorbent product changes is disruptive and/or financially prohibitive.
Condom catheter[edit | edit source]
- Effective method of urinary containment for men with severe incontinence.
- In comparison to compressive devices, condom catheter systems are acceptable for patients with any degree of urge incontinence. Theoretically, this approach would also be superior to urethral catheterization due to the avoidance of mechanical bladder irritation.
- Unsuitable for patients with
- A retractile phallus
- Skin excoriation
- Concomitant urethral stricture
- Poor manual dexterity
- A large glans/narrow phallus configuration
- The condom or sheath varies based on the material (latex or silicone), length of adhesive surface, circumference, and overall length
- Success of a condom catheter is wholly dependent on proper sizing.
Urethral catheter[edit | edit source]
- Last resort in a patient who is unsuitable for alternative management
- Suprapubic catheter drainage is not a solution for the patient with severe intrinsic sphincter deficiency, as urethral leakage will persist
Surgical[edit | edit source]
Timing[edit | edit source]
- In patients with bothersome stress urinary incontinence after prostate treatment despite conservative therapy, clinicians
- May offer surgery as early as 6 months if incontinence
- Patients who report a lack of symptom improvement or those experiencing more severe incontinence at 6months may be offered early treatment in the form of surgical interventions with such a treatment decision made using a shared decision-making model.
- Should offer surgical treatment at 12 months post-prostate treatment.
- Majority of patients will reach their maximum improvement by 12 months with minimal to no improvement afterwards.
- Withholding surgical treatment after 12 months is unlikely to result in improved patient symptoms and will delay restoration of continence.
- Conversely, treatment should be offered with caution in patients who are displaying symptom improvement.
- Majority of patients will reach their maximum improvement by 12 months with minimal to no improvement afterwards.
- May offer surgery as early as 6 months if incontinence
Pre-surgical Evaluation[edit | edit source]
- SUI should be confirmed by history, physical exam, or ancillary testing
- Demonstrate SUI on physical exam, with or without provocative testing such as bending, shifting position, or rising from seated to standing position
- Stress pad testing can also be performed.
- If there is any doubt as to whether the patient has SUI, UDS may be performed.
- Cystourethroscopy should be performed to assess for urethral and bladder pathology that may affect outcomes of surgery
- The presence of urethral pathology (e.g., stricture, vesicourethral anastomotic stenosis (VUAS), BNC, urethral lesions) may affect the outcome of surgery
- Cystourethroscopy has also been recommended prior to placement of transobturator slings to assess urethral function (patients should have visual voluntary contraction of the external sphincter), and luminal closure of the urethra should be demonstrated with bulbar compression and elevation (repositioning test). However, success of the procedure has not been shown to be dependent on these findings in any controlled study.
- Patients with symptomatic VUAS or BNC should be treated prior to surgery for IPT
- Although a VUAS or BNC will not necessarily cause SUI, treatment of them may worsen SUI. This is important because a patient may be considered for a sling procedure if he had “mild” incontinence, but he would likely need an AUS if it worsens after treatment.
- Following treatment of VUAS, an interval cystoscopy should be performed at least 4-6 weeks later to document improvement and stabilization, after which IPT treatment can be considered.
- In cases where pre-operative cystourethroscopy is not performed, it may be done at the start of the AUS or sling implantation before any incision is made.
- In such cases, patients should be made aware of the potential consequences and the possibility of aborting an AUS or sling insertion if significant urethral or bladder pathology is discovered.
- The presence of urethral pathology (e.g., stricture, vesicourethral anastomotic stenosis (VUAS), BNC, urethral lesions) may affect the outcome of surgery
- Urodynamics (UDS) may be performed in cases where it may facilitate diagnosis or counseling.
- Can aid in determining if IPT is cause by sphincter dysfunction, bladder dysfunction, or a combination of both, and also assess bladder contractility and the presence of bladder outlet dysfunction.
- UDS are not required before surgical intervention for IPT unless the clinician is in doubt of the diagnosis or it is felt that patient counseling will be affected.
- No controlled studies that assess the value of UDS versus no UDS in men with SUI prior to surgery.
- Presence of UDS abnormalities of storage (e.g., detrusor overactivity, impaired compliance, small cystometric capacity) do not affect outcomes of AUS or sling surgery in men with SUI.
- Similarly, detrusor over-activity found on UDS has not been shown to negatively impact sling outcomes in men with SUI after prostate treatment.
- Abdominal leak-point pressure has not been shown to affect outcomes of AUS
- if the clinician is unsure of how prevalent sphincteric versus bladder affecting incontinence, or if there is unexplained poor bladder emptying, then UDS may be helpful in providing that additional information. Examples of this may be
- Patient reports significant mixed incontinence and stress incontinence is not demonstrated
- Impaired compliance is suspected and incontinence could be related to high storage pressures without urgency
- Overflow incontinence is suspected (PVR) may be helpful to rule out significant retention of urine)
- ★In patients with suspected SUI who do not demonstrate SUI during UDS with a catheter in place, it is important that the catheter be removed and stress testing repeated
- Up to 35% of males with post-prostatectomy SUI will not demonstrate SUI with a catheter in place. This may be due to some scarring at the site of the anastomosis. In such cases, even a small catheter can occlude the urethra and prevent stress leakage.
Contraindications[edit | edit source]
- It is not known if poor bladder compliance and an uncorrected storage pressure are absolute contraindications to SUI surgery in IPT patients. However, these patients should be carefully followed to avoid upper tract decompensation.
- UDS likely has the highest yield for poor compliance in patients with severe radiation cystitis or those who have advanced neurogenic lower urinary tract dysfunction.
- Patients with significantly elevated storage pressures can be treated primarily (if no stress incontinence) with anticholinergics or onabotulinumtoxin A to lower such pressures. UDS then can be repeated to document adequate reservoir function
Options (5):[edit | edit source]
- Urethral bulking agents
- Adjustable balloon devices
- Slings
- AUS
- Urinary Diversion
Urethral bulking agents[edit | edit source]
- Most commonly used procedure to treat male SUI
- Considered off-label
- Currently no FDA-approved available agents for the treatment of male incontinence
Advantages[edit | edit source]
- Least invasive technique
Disadvantages[edit | edit source]
- Least effective surgical technique
- In male patients, the best success rates have been described in patients with a high Valsalva leak point pressure, unscarred vesicourethral anastomosis, and no RT history.
Indication[edit | edit source]
- Consider in patients who are unable to tolerate or refuse more invasive surgical therapy
Adjustable balloon devices[edit | edit source]
- In 2017, adjustable balloon devices became available in the United States for the treatment of male intrinsic sphincter deficiency after prostatectomy or TURP.
Advantages[edit | edit source]
- Compared to AUS (3):
- Shorter procedure length
- Less invasive placement
- Elimination of the need for patient manipulation
Disadvantages[edit | edit source]
- Higher intraoperative and early complication rates compared to other anti-incontinence procedures
- Most common intraoperative complication is urethral or bladder perforation
- Mean all-cause (i.e., erosion, infection, balloon migration or balloon failure) explantation rate is 27%, more common that AUS
- Efficacy, complication rates, and complication types have been associated with surgeon volume.
- Obtaining specialty training from an experienced implanter would be beneficial before device implantation.
Indications[edit | edit source]
- Consider for non-radiated patients with mild to moderate SUI
- RT negatively affects success and is associated with a higher complication rate.
Male slings[edit | edit source]
Indications[edit | edit source]
- Consider for mild to moderate SUI
- Might consider a sling in patients who have not undergone radiation, who have minimal incontinence at night, bothersome isolated climacturia, or who would be unable to use the AUS given poor hand function or cognitive abilities.
- Prior male sling does not typically interfere with subsequent sling revision or placement of an AUS in the setting of an unsatisfactory continence outcome.
Contraindications[edit | edit source]
- Severe SUI
- Poor efficacy in comparison to an AUS
Complications[edit | edit source]
- Generally low complication rate
- Urinary retention
- Typically resolves within 1 week
- Pelvic and perineal pain and paresthesia
- Typically resolves within 12 weeks
- Erosion and infection are rare
- If occurs, sling should should removed as soon as possible with a catheter left in place in the setting of erosion.
AUS[edit | edit source]
Indications[edit | edit source]
- Consider for mild to severe SUI
- Preferred in patients with prior (3):
- Radiation
- Patients with IPT following primary, adjuvant or salvage RT should be offered the same conservative management as a patient with postprostatectomy SUI. Patients who fail conservative measures should be offered surgical management, preferably placement of AUS.
- Radiated patients undergoing AUS placement should be counseled on potentially compromised functional outcomes and an increased risk of complications.
- Slings may be a potential option in some radiated patients but adjustable balloons are significantly less effective [different than 2019 guidelines which only supported AUS after radiation]
- Urethral reconstruction
- Urethral strictures of the anterior urethra and urethral stenosis of the posterior urethra can arise after RP, RT, or treatment for IPT. Urethral reconstructive surgery is often used to treat narrowing in the urethra.
- Male slings will not be effective given post-surgical changes related to most types of urethral reconstruction in the posterior and anterior urethra
- Complications rates are higher
- Depending on the technique employed (urethra transecting or not) the blood supply to the urethra may be diminished and potentially decrease the life span of an AUS.
- Vesicourethral anastomotic stenosis or bladder neck contracture
- Decreased success rates when undergoing male slings
- Radiation
Contraindications[edit | edit source]
- Inadequate physical or cognitive abilities to operate the device
- Should be some assurance that patients can physically pump a device that is in a normal position in the scrotum.
- There are no uniform ways to demonstrate such dexterity, but a simple demonstration of strength in the fingers and the ability to squeeze the pump between the index finger and thumb should be minimal requirements.
- Should be some assurance that patients can physically pump a device that is in a normal position in the scrotum.
Procedure[edit | edit source]
- Approach: single cuff perineal approach is preferred
- Superior outcomes compared to transverse scrotal incision, likely due to a more distal cuff placement, and reduced risk of complications and need for revision
- Similar outcomes compared to tandem cuff placement but reduced risk of complications
Complications[edit | edit source]
- Intraoperative urethral injury
- If identified during implantation, procedure should be abandoned and subsequent implantation should be delayed
- Persistent leakage
- Erosion
- Infection
- Mechanical failure
- Decreased efficacy over time and reoperations are common
- The current version consists of a hydraulic system composed of 3 separate parts:
- A urethral cuff of varying sizes
- A pressure regulating balloon reservoir with three available pressure profiles
- A control pump
- The device will fail if any of the 3 parts, the tubing, or connections suffer a micro-perforation with loss of fluid
- The rate of device failure increases with time, with failure rates of
- ≈24% at 5 years
- ≈ 50% at 10 years
- AUS might need to be replaced over time due to persistent or recurrent incontinence generally due to (3):
- Urethral atrophy
- Improper cuff sizing
- Partial fluid loss
- A malfunctioning AUS does not necessarily need to be replaced, but if the patient is healthy and requests a replacement, the AUS can be explanted and a new one replaced at the same operative setting.
- The durability and efficacy of a secondary re-implant in this setting is the same as that of a primary AUS, except in the setting of erosion
- The current version consists of a hydraulic system composed of 3 separate parts:
- Risk factors for complications
- Radiation
- Urethral compromise
- Can be due to surgical intervention, including urethroplasty, multiple treatments for BNC or stricture, urethral stent placement, and prior AUS erosion1
Urinary diversion[edit | edit source]
- Can be considered in patients who are unable to obtain long-term quality of life due to incontinence after prostate treatment.
- In patients who are unable to obtain a satisfactory QoL long-term with an AUS due to multiple device failures, intractable BNC, or severe detrusor instability, urinary diversion with or without cystectomy may be an option
- If bladder preservation is feasible, conversion to a Mitrofanoff (e.g. Appendix, Monti), incontinent ileovesicostomy, or suprapubic tube with bladder neck closure may confer an improved QoL.
- In the event of the “hostile” bladder, cystectomy in combination with either an ileal conduit or continent catheterizable pouch would best manage incontinence while protecting the upper tracts.
Other[edit | edit source]
- Other potential treatments for IPT should be considered investigational
- Promising results reported in small case series for interventions such as extracorporeal magnetic intervention and penile vibratory stimulation.
Special Situations[edit | edit source]
Persistent Incontinence after Surgery (AUS or sling)[edit | edit source]
Diagnosis and Evaluation[edit | edit source]
- Same as prior: history + physical exam +/- other investigations to determine the cause of incontinence
Causes (5)[edit | edit source]
- Inadvertently deactivating the device
- Re-education must be performed
- Acute fluid loss
- The volume in the pressure regulating balloon can be assessed using computerized tomography or ultrasound.
- Poor cuff coaptation
- Cuff coaptation may be evaluated by cycling the device during cystoscopic visualization.
- Although rare, poor coaptation in the absence of fluid loss in the early post-operative phase is related to improper cuff sizing or incomplete engagement of the cuff tab.
- Either situation can only be addressed by operative revision.
- Wear or urethral atrophy
- Recurrent incontinence after years of normal function suggests either development of a new leak due to wear or urethral atrophy
- Cystoscopy is the mainstay for evaluation of atrophy and erosion.
- A leak can be confirmed by decreased volume in the pressure regulating balloon, which can be assessed by using ultrasound or computerized tomography.
- Recurrent incontinence after years of normal function suggests either development of a new leak due to wear or urethral atrophy
- Elevated storage pressures or detrusor over-activity
- Should be suspected in a patient with a normally functioning AUS
- UDS may be performed to evaluate filling pressures, capacity, presence of uninhibited detrusor contractions, and effective voiding.
- As a technical point, the cuff needs to be temporarily deflated and deactivated to allow for safe and atraumatic urodynamic sensor placement. If there are concerns regarding cuff damage, cystoscopy must be performed immediately to evaluate.
- In all cases of detrusor dysfunction, the underlying abnormalities must be addressed rather than performing any adjustments to the AUS with the exception of deflating and deactivating in the patient experiencing retention.
Management[edit | edit source]
- For persistent or recurrent SUI after
- Sling, an AUS is recommended
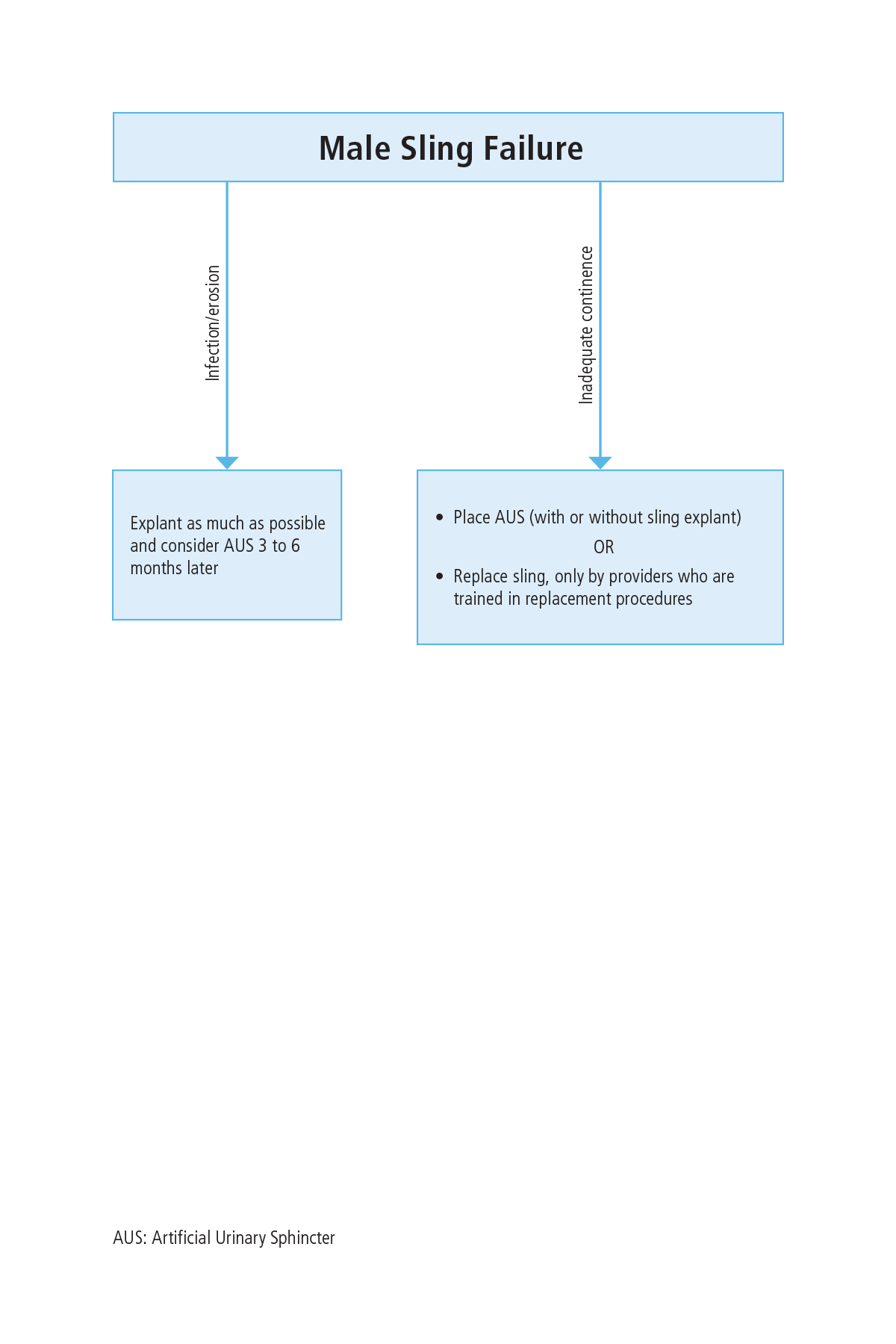
- Failure of a male sling can be due to infection or erosion, or more likely, due to patient dissatisfaction with continence recovery
- AUS, revision should be considered
- Inadequate recovery of continence after AUS placement can be due to a host of factors, including suboptimal cuff sizing at the time of original operation or inadequate pressure regulating balloon gradient.
- In patients with a possible distally located cuff, or those with a larger cuff, proximal relocation or downsizing of the cuff are both reasonable options and will likely lead to better continence.
- Tandem cuff placement is the addition of a cuff to the original cuff and has also been shown to be effective as a salvage procedure for patients with persistent incontinence.
- Specific additional risks of tandem cuff placement should be discussed with the patient prior to proceeding, including injury to the urethra during dissection, which would lead to aborting the case and the higher risk of subsequent erosion.
- Sling, an AUS is recommended
Patients presenting with infection or erosion of AUS or sling[edit | edit source]
- Erosion
- A devastating complication that can lead to urine extravasation, infection, abscess formation and sepsis, and may result in long-term urethral fistula, urethral diverticula, or urethral stricture after AUS explant.
- Incidence
- Occurs in 1-10% of cases on long-term follow-up
- Pathophysiology
- Can be due to unrecognized urethral injury at the time of initial surgery or more likely due to subsequent instrumentation of the urethra including catheterization.
- Diagnosis and Evaluation
- Generally presents with with hematuria, dysuria, or difficulty emptying the bladder and is diagnosed with a cystoscopic demonstration of the AUS cuff within the urethra
- Management:
- Explanting eroded device with urethral catheter alone, in situ urethroplasty, or anastomotic urethroplasty
- During explant, the goal of erosion management is to maximize the chances of urethral healing without developing a fistula or stricture.
- The degree of urethral loss with erosion can be highly variable, ranging from a small <5mm hole in the urethra, to complete circumferential urethral loss under the 2cm cuff.
- The urethral defect will usually heal by leaving a urethral catheter in place for 3 weeks.
- Some authors, however, recommend a urethral repair in cases of larger urethral defects due to decreased rates of stricture. The decision on how to best manage the erosion takes into consideration the size of the urethral defect, quality of local tissues (there are heterogeneous degrees of inflammation, induration, and fibrosis), and surgeon preference/experience.
- Explanting eroded device with urethral catheter alone, in situ urethroplasty, or anastomotic urethroplasty
- Infection
- Often times an infection is secondary to a pre-existing erosion.
- AUS isolated cuff infections are rare without an associated erosion.
- Incidence
- Device infection occurs in <1-5% of cases
- Diagnosis and Evaluation
- History and Physical Exam
- Presents with (4):
- Pain at the site of the AUS
- Fever
- Scrotal warmth or erythema
- Skin changes
- Presents with (4):
- History and Physical Exam
- Management:
- Explantation should be performed as soon as possible
- Timing of removal is usually influenced by severity of the infection and acuity of the clinical situation as indicated by the associated signs and symptoms (e.g., purulent drainage, erythema, tenderness, fever, chills).
- In the case of the AUS, the most conservative course of action is removal of all components, regardless of whether the infection and any associated reaction are limited to a single component.
- An infected male sling should be removed as completely as feasible without damaging any adjacent structures.
- Explantation should be performed as soon as possible
- Often times an infection is secondary to a pre-existing erosion.
- For patients seeking a replacement device (AUS or male sling) after infection and/or erosion, a waiting period of 3-6 months is recommended.
- In the AUS patient, it may be necessary to proceed with transcorporal placement of the cuff to place the cuff at a different location along the urethra.
Sexual arousal incontinence or climacturia[edit | edit source]
- As with post-prostatectomy SUI, for those with sexual arousal incontinence or climacturia, conservative management (dehydration and emptying the bladder prior to sex, use of condoms to catch the urine, achieving orgasm while supine, and PFME) should be the initial treatment
- Imipramine, a tricyclic antidepressant, has been used, but this medication is generally contraindicated in men age > 65 due to the risk of somnolence, falling down, and changes in cognition.
- The use of a penile variable tension loop (a soft silicone tube placed around the penis and adjusted to provide pressure on the urethra to physically prevent leaking during sex) has been used with success
- Both the AUS and the trans-obturator male sling, when implanted for SUI, are associated with high rates of improvement in climacturia
Concomitant IPT and erectile dysfunction[edit | edit source]
- In patients with concomitant IPT and erectile dysfunction, a concomitant or staged procedure may be offered.
- Concomitant surgery is safe
- Rate of device infection, erosion or malfunction was not increased in combined compared to staged procedures.
- Similar continence, sexual function, and overall satisfaction in patients undergoing staged versus combined procedures
- Concomitant surgery is safe
Questions[edit | edit source]
- What is the guideline-based definition of urinary continence?
- What are risk factors for incontinence after RP?
- When are patients expected to achieve their maximum continence after RP?
- What is the workup for a patient presenting with incontinence after RP?
- What are non-surgical/surgical treatment options for IPT?
- When should surgical intervention be performed in a patient with bothersome incontinence after RP?
- Are any investigations needed prior to surgical intervention for incontinence after RP?
- What is the management of AUS cuff erosion?
- Which surgical treatment is preferred in patients with previous history of pelvic radiation?
- What are potential causes for persistent incontinence after surgical treatment?
- A patient previously treated with sling for incontinence after RP has persistent bothersome incontinence. What is the next treatment?
Answers[edit | edit source]
- What is the guideline-based definition of urinary continence?
- Not requiring a pad or protective device to stay dry (pad-free)
- What are risk factors for incontinence after RP?
- Older age
- Larger prostate size
- Shorter membranous urethral length
- Preservation of NVB at time of RP
- When are patients expected to achieve their maximum continence after RP?
- 12 months
- What is the workup for a patient presenting with incontinence after RP?
- H+P +/- PVR [likely U/A, though not mentioned in guidelines]
- What are non-surgical/surgical treatment options for IPT?
- Non-surgical: PFMT/PFME +/- penile compression devices, pads, condom catheter, urethral catheter
- Surgical: bulking agents, inflatable-balloon devices, male sling, AUS
- When should surgical intervention be performed in a patient with bothersome incontinence after RP?
- 12 months, unless patient prefers to be done at 6
- Are any investigations needed prior to surgical intervention for incontinence after RP?
- Objective confirmation of SUI
- Cystourethroscopy
- What is the management of AUS cuff erosion?
- AUS explant with urethral catheter left in place for a few weeks; AUS should not be reimplanted for 3 months
- Which surgical treatment is preferred in patients with previous history of pelvic radiation?
- AUS
- What are potential causes for persistent incontinence after surgical treatment?
- Patient self-deactivating device
- Fluid loss from system
- Urethral atrophy
- OAB
- A patient previously treated with sling for incontinence after RP has persistent bothersome incontinence. What is the next treatment?
- AUS
References[edit | edit source]
- Sandhu, Jaspreet S., et al. "Incontinence after prostate treatment: AUA/SUFU guideline." The Journal of urology 202.2 (2019): 369-378.