(97 intermediate revisions by the same user not shown)
Line 1:
Line 1:
'''See [https://www.ncbi.nlm.nih.gov/pubmed/28401957 Contemporary management of patients with penile cancer and lymph node metastasis] (Nat Rev Urol 2007)'''
'''See [https://www.ncbi.nlm.nih.gov/pubmed/28401957 Contemporary management of patients with penile cancer and lymph node metastasis] (Nat Rev Urol 2007)'''
== Indications ==
# '''<span style="color:#ff0000">Clinically node-positive disease (palpable on physical exam)</span>'''
# '''<span style="color:#ff0000">Clinically node-negative disease (not palpable on physical exam) but increased risk for inguinal metastasis based on primary tumor characteristics (pT ≥2, presence of vascular or lymphatic invasion, or grade ≥3).</span>'''
#* '''cN3 (fixed nodal mass) is managed initially with neoadjuvant chemotherapy followed by radical inguinal lymphadenectomy in responders'''
* '''<span style="color:#ff0000">May be curative when the disease is limited to the inguinal nodes.</span>'''
== Anatomic Considerations ==
== Anatomic Considerations ==
=== Femoral Triangle ===
* '''See [[Anatomy: Groin and Inguinal|Groin and Inguinal Anatomy Chapter Notes]]'''
**'''<span style="color:#ff0000">Drains the glans penis</span>'''
**'''<span style="color:#ff0000">Empties into the superficial inguinal nodes and the deep inguinal nodes</span>'''
*'''Primary site of metastatic spread of penile carcinoma occurs via the regional lymphatic system, first to the inguinal lymph node chain and then to the iliac and pelvic lymph nodes.'''
** '''Penetration of Buck’s fascia or the tunica albuginea by the primary penile tumor allows for dissemination of tumor cells into the lymphatic system'''
**Presence and extent of regional LN metastases is the single most important prognostic factor in determining the long-term survival of patients with penile cancer
***If cancer has spread to the pelvic nodes, long-term survival is < 10%
**'''Inguinal metastatic spread can be unilateral or bilateral'''
***Crossover drainage from the right to left groin or vice versa can also occur
**Metastatic spread from the inguinal lymph nodes to the contralateral pelvis or from the right to left pelvis has never been reported.
**'''Skip lesions with direct lymphatic drainage from penile tumors to the pelvic lymph nodes has never been reported.'''
**Further spread from the true pelvis to the retroperitoneal lymph nodes is beyond the regional drainage system of the penis and represents systemic metastatic disease
== Open Inguinal Node Dissection ==
==== Borders ====
=== Videos ===
* '''<span style="color:#ff0000">Roof: fascia lata (covers femoral sheath)'''
*[https://www.youtube.com/watch?v=5HdhCDdDnP0 Video 1 (Dr. Franco Gaboardi)]
*In patients with pre-operative cellulitis or infection of the groin region, oral antibiotics (i.e., usually a 1st generation cephalosporin or penicillin) to treat and control this infection prior to surgical management is strongly advised.[https://pubmed.ncbi.nlm.nih.gov/18762945/]
**Divides into superficial femoral artery and deep (profunda) femoral artery
**If the primary tumor is infected, Inguinal lymphadenectomy is best performed in a staged fashion n order to remove the infected source and provide appropriate antibiotic coverage based upon the clinical circumstances
**'''Blood supply to the skin of the inguinal region is from branches of the common femoral artery. Complete inguinal dissection necessitates ligation of these branches.'''
***'''Viability of the skin flaps raised during the dissection depends on anastomotic vessels in the superficial fatty layer of the Camper fascia'''
**'''<span style="color:#ff0000">Medial to femoral nerve</span>'''
** '''<span style="color:#ff0000">Drains the glans penis</span>'''
** '''<span style="color:#ff0000">Empties into the superficial inguinal nodes and the deep inguinal nodes</span>''' '''<span style="color:#ff0000">of the femoral triangle</span>'''
* '''<span style="color:#ff0000">Penile cancer can metastasize to the contralateral inguinal nodes</span> because of crossover in the symphyseal region'''
* '''<span style="color:#ff0000">Drainage subsequently proceeds from the inguinal nodes to the ipsilateral pelvic lymph nodes'''
** If the tumor has spread to the pelvic nodes, long-term survival is < 10%
*Because lymphatic drainage of the penis to the groin runs beneath the Camper fascia, '''Camper’s fascia can be preserved and left attached to the overlying skin''' when the superior and inferior skin flaps are fashioned. '''On the basis of this anatomy, a transverse skin incision least compromises this blood supply.'''
== Inguinal Lymphadenectomy ==
* '''Thighs slightly abducted and externally rotated (frog-leg[https://pubmed.ncbi.nlm.nih.gov/30730389/]) with cushioned support under the flexed knee.'''
* '''In the standard radical inguinal lymphadenectomy, both the superficial and deep inguinal lymph nodes are removed'''
==== Incision ====
** '''Superficial dissection removes nodes superficial to the fascia lata'''
=== Indications ===
* '''Oblique incision ≈2-3 cm below and parallel to the inguinal ligament (groin crease)[https://pubmed.ncbi.nlm.nih.gov/21481617/]'''
# '''<span style="color:#ff0000">Clinically node-positive disease (palpable on physical exam)</span>'''
**'''Lateral end'''
# '''<span style="color:#ff0000">Clinically node-negative disease (not palpable on physical exam) but increased risk for inguinal metastasis based on primary tumor characteristics (pT ≥2, presence of vascular or lymphatic invasion, or grade ≥3).</span>'''
***'''Radical inguinal lymphadenectomy: line drawn from the anterior superior iliac spine extending inferiorly'''
#* '''cN3 (fixed nodal mass) is managed initially with neoadjuvant chemotherapy followed by radical inguinal lymphadenectomy in responders'''
***'''Modified inguinal lymphadenectomy: vertical line drawn from above the femoral artery'''
**'''Medial end'''
***'''Radical or modified inguinal lymphadenectomy: line drawn from the pubic tubercle extending inferiorly'''
*Special scenario: When the overlying skin is involved with disease secondary to direct tumor invasion or broken down by infection or prior therapy and requires excision, consider an elliptical incision with resection of the involved skin and the subcutaneous tissue[https://pubmed.ncbi.nlm.nih.gov/27717432/]
**In this setting, the incision may alternatively be extended superiorly from the lateral border of the ellipse and inferiorly from the medial border to make a single S-shaped incision for the iliac and inguinofemoral dissections
* '''<span style="color:#ff0000">May be curative when the disease is limited to the inguinal nodes.</span>'''
=== Standard radical inguinal lymphadenectomy ===
*'''In the standard radical inguinal lymphadenectomy, both the superficial and deep inguinal lymph nodes are removed'''
* '''<span style="color:#ff0000">Superior: inguinal ligament/superior boundary of the external oblique aponeurosis and the spermatic cord</span>'''
** '''<span style="color:#ff0000">Boundaries of dissection:</span>'''§
**'''<span style="color:#ff0000">Inguinal ligament is the portion of the external oblique aponeurosis which extends between the anterior superior iliac spine and the pubic tubercle as a thick band, folded inward[https://en.wikipedia.org/wiki/Aponeurosis_of_the_abdominal_external_oblique_muscle]</span>'''
* '''<span style="color:#ff0000">Lateral: sartorious muscle</span> (saphenous vein and femoral vein in modified template)[https://pubmed.ncbi.nlm.nih.gov/16643509/]'''
*** '''<span style="color:#ff0000">Lateral: sartorious muscle</span> (saphenous vein and femoral vein in modified template)'''
* '''<span style="color:#ff0000">Inferior: apex of the femoral triangle/fossa ovalis (where the saphenous penetrates the fascia lata)</span>'''
*** '''<span style="color:#ff0000">Inferior: apex of the femoral triangle/fossa ovalis (where the saphenous penetrates the fascia lata)</span>'''
*'''<span style="color:#ff0000">Floor: pectineus muscle for deep dissection (fascia lata for superficial)</span>'''
** '''Position: involved thigh slightly abducted and externally rotated with cushioned support under the flexed knee.'''
**Note that adductor longus and sartorious are posterior to fascia lata and are therefore not the relevant medial and lateral boundaries for superficial dissection.
** '''Incision'''
==== Step by step ====
*** The inguinofemoral dissection is designed to cover an area outlined superiorly by a line drawn from the superior margin of the external ring to the anterior superior iliac spine, laterally by a line drawn from the anterior superior iliac spine extending 20 cm inferiorly, and medially by a line drawn from the pubic tubercle 15 cm down the medial thigh.
* See [https://pubmed.ncbi.nlm.nih.gov/16643509/ BJUI Surgical atlas. Surgical management of penile carcinoma: the inguinal nodes]
*** In most situations the procedure is carried out through an oblique incision approximately 3 cm below and parallel to the inguinal ligament and extending from the lateral to the medial limit of the dissection (Fig. 39-21).
*'''General anesthesia and insertion of lines.''' No need for naso/orograstric tube for gastric decompression during case.
*** If an area of the skin overlying the cancer-bearing nodes is invaded or adherent and requires excision, an elliptical incision is made around the involved skin and then extended medially and laterally. In this setting, the incision may alternatively be extended superiorly from the lateral border of the ellipse and inferiorly from the medial border to make a single S-shaped incision for the iliac and inguinofemoral dissections
** '''Superior and inferior skin flaps are developed in the plane just below the Scarpa fascia.'''
** After induction of general anesthesia...
*** The superior flap is elevated cephalad to a point 4 cm above the inguinal ligament, and the inferior flap to the limit of the dissection.
** Trim hair overlying operative site, if needed
** The fat and areolar tissues are dissected from the external oblique aponeurosis and the spermatic cord to the inferior border of the inguinal ligament, forming the superior boundary of the lymph node packet
** Insert 16-Fr Foley catheter
** '''The inferior angle of the inguinofemoral exposure is at the apex of the femoral triangle, where the long saphenous vein is identified and divided.'''
** Externally rotate the hip and flex the knee. Place cushioned support under the flexed knees.
*** '''In patients with minimal metastatic disease, it may be feasible and beneficial to spare the saphenous vein, and this should be considered to attempt to decrease the risk of lower-extremity complications.'''
** Prepare area with chlorhexidine–alcohol scrub
** Dissection is deepened through the fascia lata overlying the sartorius muscle laterally and the thinner fascia covering the adductor longus muscle medially. At the apex of the femoral triangle, the femoral artery and vein are identified, and dissection is continued superiorly along the femoral vessels. Superficial cutaneous perforating arteries are ligated as they are encountered on the surface of the femoral artery. The saphenous vein is divided at the saphenofemoral junction, and the dissection is continued superiorly to include the deep inguinal nodes medial and lateral to the femoral vein until continuity with the pelvic dissection is attained at the femoral canal
***Preoperative skin preparation with a chlorhexidine–alcohol scrub provided a significantly lower surgical site infection rate at 30 days when compared to a skin prep with a povidone–iodine solution
** '''The anterior aspects of the femoral vessels are dissected, but the femoral vessels are not skeletonized, and the lateral surface of the femoral artery is not exposed.'''
**Drape with exposure of the umbilicus, pubic tubercle, anterior superior iliac spine, and anterior thigh
*** '''This avoids injury to the femoral nerve and the profunda femoris artery'''
*'''Use marking pen to denote landmarks and incision.'''
**** '''The femoral nerve is usually not visible as it runs beneath the iliacus fascia lateral to the femoral artery.'''
** Landmarks
** '''After the femoral triangle is dissected the sartorius muscle is mobilized from its origin at the anterior superior iliac spine and either transposed or rolled 180 degrees medially to cover the femoral vessels.'''
*** Anterior superior iliac spine
*** The muscle is sutured to the inguinal ligament superiorly, and its margins are sutured to the muscles of the thigh immediately adjacent to the femoral vessels
*** Pubic tubercle
** The femoral canal is closed, if necessary, by suturing the shelving edge of the Poupart ligament to the Cooper ligament, being careful not to compromise the lumen of the external iliac vein or to injure the inferior epigastric vessels in the process.
****If middle finger is on pubic symphysis, index finger is on pubic tubercle
** '''Closure'''
*** Inguinal ligament (line from anterior superior iliac spine to pubic tubercle)
*** Primary closure of the inguinofemoral dissection is usually possible with minimal or no further mobilization of the excision margins.
***Femoral artery (if palpable, usually located approximately at the midpoint of the inguinal ligament)
***Fossa ovalis/saphenous opening (3–4 cm inferior and lateral to the pubic tubercle)
**Lateral end of incision is to a line drawn from the anterior superior iliac spine extending inferiorly and the medial end of the incision is to a line drawn from the pubic tubercle extending inferiorly
***The boundaries of dissection in a radical inguinal lymphadenectomy are defined by the superior margin of the external ring to the anterior superior iliac spine, laterally from the anterior superior iliac spine extending 20 cm inferiorly and medially to a line drawn from the pubic tubercle 15 cm downward[https://pubmed.ncbi.nlm.nih.gov/21481617/]
*'''Develop and raise superior and inferior skin flaps'''
**'''Use left hand to retract and Metzenbaum scissors/cautery to develop and raise superior and inferior skin flaps below Camper's fascia down to the level of the external oblique aponeurosis to expose the inferior border of the inguinal ligament and spermatic cord.'''
*** '''Important to leave a 6—8 mm thickness of subcutaneous tissue in contact with the skin to avoid necrosis[https://www.sciencedirect.com/science/article/pii/S1878788623000292]'''
****Care should be taken to preserve the superficial blood supply to the flaps, thus minimizing the risk of postoperative skin necrosis, infection, and wound breakdown
****Camper’s fascia can be preserved and left attached to the overlying skin when the superior and inferior skin flaps are fashioned.
*****Lymphatic drainage of the penis to the groin runs beneath the Camper fascia
*****Camper's fascia may appear as glistening layer
***Superior skin and subcutaneous tissue flap is developed ≈8 cm superiorly'''[https://pubmed.ncbi.nlm.nih.gov/21481617/]''' towards the inguinal ligament
****Spermatic cord if reflected medially[https://www.youtube.com/watch?v=5HdhCDdDnP0]
***Inferior skin and subcutaneous tissue flap is developed ≈6 cm inferiorly'''[https://pubmed.ncbi.nlm.nih.gov/21481617/]'''
***Develop flap medially to adductor longus aponeurosis
***Develop flap laterally to sartorious
**'''Handle the skin flap edges gently[https://pubmed.ncbi.nlm.nih.gov/27717432/]'''
***'''Assistant uses hooks initially and army navy retractors later to lift up on skin edge'''
***Avoid grasping of the flap edges with forceps because this could potentially crush and devascularize the tissue.
***Consider covering skin flap edges with saline-moistened sponges
**'''Reflect the spermatic cord medially'''
*'''Lymph node dissection'''
**'''Use titanium surgical clips, absorbable suture, or LigaSure for meticulous control of lymphatic channels to avoid a lymphatic leak.<span style="color:#ff0000">[https://link.springer.com/content/pdf/10.1007/978-1-62703-367-1.pdf]</span>'''
**'''The first landmark in the inguinal node dissection is the saphenous vein[https://pubmed.ncbi.nlm.nih.gov/16643509/]'''
**'''Superficial lymph node dissection'''
***'''Remove lymphatic tissue above the fascia lata[https://pubmed.ncbi.nlm.nih.gov/27717432/]'''
****Fascia lata is continuous with Scarpa fascia superiorly, transitions at inguinal ligament
***'''Majority of the lymph nodes will be found in the central and medial zones[https://pubmed.ncbi.nlm.nih.gov/30730389/]'''
****Anatomic lymph groups (5) by location:
****#'''Central nodes around the saphenofemoral junction'''
****#'''Superomedial nodes''' around the superficial external pudendal and superficial epigastric veins
****##'''Drain the prepuce of the penis and the scrotum'''
****#'''Inferomedial nodes around the greater saphenous vein'''
****#Superolateral nodes around the superficial circumflex vein
****#Inferolateral nodes around the lateral femoral cutaneous and superficial circumflex veins
****In obese patients, it may be easy to overlook the superior medial zone nodal tissue if a prominent suprapubic fat pad is present.
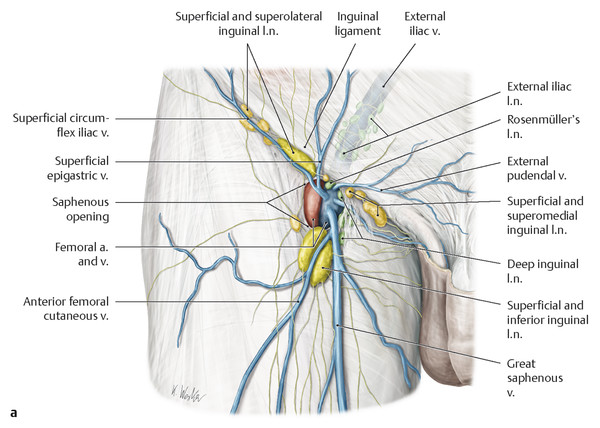
***'''Identify and ligate veins in this area''', which can include (see [https://radiologykey.com/wp-content/uploads/2017/12/978-1-62623-013-2_c001_f006a.tif_epub1.jpg Figure])
****Superficial epigastric vein (drains into the greater saphenous vein proximally) at the superior boundary of dissection
****Superficial circumflex iliac vein (drains into the greater saphenous vein laterally) at the superior boundary of dissection
****External pudendal vein (drains into the greater saphenous vein medially)
****Anterior/lateral accessory saphenous vein (drains into the greater saphenous vein laterally)
***Superior boundary: dissect the fat and areolar tissues to the level of the external oblique fascia, the external inguinal ring, and the exposure of the spermatic cord
****Ligate and divide the first lymphatic packet: a funiculus of lymphofatty tissue, extending from the base of the penis to the superomedial portion of this lymph node packet[https://link.springer.com/content/pdf/10.1007/978-1-62703-367-1.pdf][https://pubmed.ncbi.nlm.nih.gov/21481617/]
****Then from the iliac bone, then from the inguinal ligament (this should expose the femoral vessels)[https://www.youtube.com/watch?v=5HdhCDdDnP0]
*** Inferior boundary: inferior angle of the inguinofemoral exposure at the apex of the femoral triangle
*** Lateral boundary: anterior superior iliac spine (circumflex iliac vessels that can be ligated)[https://www.youtube.com/watch?v=5HdhCDdDnP0]
**'''Identify the Great saphenous vein at the inferior boundary of the femoral triangle'''
***'''Great saphenous vein approaches common femoral vein medially'''
***In standard radical inguinal lymphadenectomy, the great saphenous vein and the lateral saphenous vein are divided at the saphenofemoral junction. However, this increases the risk of lower-extremity complications
***In modified inguinal lymphadenectomy (see below), the Great saphenous vein is spared.
****In patients with minimal metastatic disease, it may be feasible and beneficial to spare the saphenous vein.
***Medial boundary: Dissect medially to identify the aponeurosis of the adductor longus muscle of the thigh
***Lateral boundary: Dissect laterally to identify the aponeurosis of the sartorius muscle [or up to the circumflex iliac vessels
** '''Deep lymph node dissection'''
***'''Enter the fascia lata'''
****'''Overlying the sartorius muscle laterally and medially through the thinner fascia of the adductor longus muscle[https://link.springer.com/book/10.1007/978-1-4939-6679-0]'''
****At the level of the saphenous opening[https://pubmed.ncbi.nlm.nih.gov/30730389/]
*****Lies 3-4cm below and lateral to the pubic tubercle
*****Transmits the great saphenous vein and other smaller vessels including the superficial epigastric artery and superficial external pudendal artery, as well as the femoral branch of the genitofemoral nerve[https://en.wikipedia.org/wiki/Saphenous_opening]
***'''Identify the femoral artery and vein at the apex of the femoral triangle. Use the femoral vessels to guide the dissection along superiorly[https://pubmed.ncbi.nlm.nih.gov/21481617/]'''
****'''The anterior aspects of the femoral vessels are dissected, but the femoral vessels are not skeletonized, and the lateral surface of the femoral artery is not exposed.[https://pubmed.ncbi.nlm.nih.gov/21481617/]'''
***** '''This avoids injury to the femoral nerve and the deep femoral artery'''
****** '''The femoral nerve is usually not visible as it runs beneath the iliacus fascia lateral to the femoral artery.'''
******Branches of the femoral nerve can be on the lateral border of the femoral artery, which must be preserved.
*****'''Be careful when dissecting over the femoral vessels'''
***'''Continue dissection superiorly along the anterior surface of the femoral vein and the femoral artery working medially to laterally over the femoral vein and artery up to the inguinal ligament''' until the femoral canal is reached where continuity to the pelvic dissection is attained to include the deep inguinal nodes.
****The femoral canal is located medial to the femoral vein below the inguinal ligament
****Superficial cutaneous perforating arteries are ligated as they are encountered on the surface of the femoral artery.
***'''Use both blunt and sharp dissection to resect the deep inguinal nodes.'''
****The deep nodes are typically no more than 3–5 lymph nodes contained within the femoral sheath[https://pubmed.ncbi.nlm.nih.gov/30730389/]
*****The node of Cloquet is the most proximal in the femoral canal and considered the margin between the inguinal and pelvic lymph nodes[https://pubmed.ncbi.nlm.nih.gov/30730389/]
******Cloquet’s lymph node is removed.
***'''Clip and transect specimen at the level of the femoral canal'''
**'''Send intraoperative frozen section of lymph node packet'''
***Intraoperative frozen section has been shown to have diagnostic value in determining the need to proceed to a radical dissection[https://pubmed.ncbi.nlm.nih.gov/30730389/]
***It may be time-saving to proceed to the contralateral dissection while awaiting frozen section results.
*'''Apply sartorius flap, if needed, for''' '''coverage over the femoral vessels and nerves'''
**'''If a deep dissection, the sartorius muscle can be transposed or rolled 180 degrees medially by releasing its attachments from the anterior superior iliac spine, providing myocutaneous coverage over the femoral vessels and nerves'''
***The sartorius flap is sutured to the inguinal ligament superiorly with interrupted 2-0 Vicryl sutures, and its margins are sutured to the muscles of the thigh immediately adjacent to the femoral vessels[https://pubmed.ncbi.nlm.nih.gov/21481617/]
*'''Closure'''
** '''Irrigate the wound'''
*** Irrigate aggressively with water or saline using a bulb syringe to remove small clots and uncover a potential bleeding source.[https://pubmed.ncbi.nlm.nih.gov/18762945/]
** '''Insert multiperforated closed-suction drains (10 or 15 French)'''
*** Place drains under the subcutaneous tissue in the dissected area along the femoral vascular axis[https://www.sciencedirect.com/science/article/pii/S1878788623000292] and bring the drains out inferiorly, to prevent lymphocele formation.
** Primary closure of the inguinofemoral dissection is usually possible with minimal or no further mobilization of the excision margins.
*** When circumstances demand a large area of inguinal soft tissue sacrifice, primary closure may be obtained by scrotal skin rotation flaps an abdominal wall advancement flap or a myocutaneous flap based on the rectus abdominis or tensor fasciae latae for more extensive defects.
*** When circumstances demand a large area of inguinal soft tissue sacrifice, primary closure may be obtained by scrotal skin rotation flaps an abdominal wall advancement flap or a myocutaneous flap based on the rectus abdominis or tensor fasciae latae for more extensive defects.
*** '''Closed-suction drains''' are placed under the subcutaneous tissue and brought out inferiorly.
** Suture skin flips to the surface of the exposed musculature to decrease dead space.
*** During closure, the skin flaps are sutured to the surface of the exposed musculature to decrease dead space.
***This can minimize the risk of a postoperative fluid collection (i.e., seroma) that may serve as a potential source for infection.
*** The skin is closed with absorbable subcutaneous sutures and staples.
**Reapproximate subcutaneous tissues with 2-0 Vicryl
** '''Post-operative care'''
**Reapproximate skin with 3-0 non-absorbable suture or skin staples[https://www.sciencedirect.com/science/article/pii/S1878788623000292]
*** '''The patient is maintained on bed rest for 2 or 3 days, and pneumatic compression stockings are used.'''
**Apply dressings
*** '''Efforts to minimize lymphedema during the initial postoperative period include applying thigh-high elastic wraps or stockings and elevating the foot of the bed.'''
*** The drains are removed after 5 to 7 days, when drainage is less than 30 to 40 mL/day.
'''Advantage'''
*** We maintain the patient on a suppressive dose of a cephalosporin for 1 to 2 months until healed to decrease the incidence of erythema and cellulitis, and this seems to improve overall wound healing.
*'''Less morbidity than standard radical inguinal lymphadenectomy'''
###Also known as the saphenous opening[https://en.wikipedia.org/wiki/Saphenous_opening]
*** '''Strong risk factor for complications is palliative indication for ILND'''§
###An oval opening in the upper mid part of the fascia lata of the thigh
###Allow the passage of the great saphenous vein
###Lies 3–4 cm below and lateral to the pubic tubercle and is about 3 cm long and 1.5 cm wide.
# '''<span style="color:#ff0000">Preservation of the saphenous vein[https://pubmed.ncbi.nlm.nih.gov/30730389/]</span>''' and lateral accessory saphenous vein[https://www.youtube.com/watch?v=5HdhCDdDnP0]
##Superficial epigastric and superficial circumflex veins are ligated at the superior boundaries of dissection[https://www.youtube.com/watch?v=5HdhCDdDnP0]
##Superficial epigastric, superficial circumflex veins, external pudendal veins are ligated at the superior boundaries of dissection[https://www.youtube.com/watch?v=5HdhCDdDnP0]
# '''<span style="color:#ff0000">Elimination of the need to transpose the sartorius muscle[https://pubmed.ncbi.nlm.nih.gov/30730389/]</span>'''
* '''Less morbidity than standard inguinal lymphadenectomy'''
*'''<span style="color:#ff0000">Clinically node-negative disease (not palpable on physical exam) but increased risk for inguinal metastasis based on primary tumor characteristics (pT ≥2, presence of vascular or lymphatic invasion, or grade ≥3).</span>'''
* '''<span style="color:#ff0000">Key aspects of the procedure are (5):</span>'''
==== Boundaries of Dissection[https://pubmed.ncbi.nlm.nih.gov/16643509/ §] ====
*# '''<span style="color:#ff0000">Limiting dissection by excluding the area lateral to the saphenous vein and femoral vein</span>'''§
* '''<span style="color:#ff0000">Superior: inguinal ligament/superior boundary of the external oblique aponeurosis and the spermatic cord</span>'''
*#* Lateral limit of dissection saphenous and femoral vein in modified dissection
**'''<span style="color:#ff0000">Inguinal ligament is the portion of the external oblique aponeurosis which extends between the anterior superior iliac spine and the pubic tubercle as a thick band, folded inward[https://en.wikipedia.org/wiki/Aponeurosis_of_the_abdominal_external_oblique_muscle]</span>'''
*# '''<span style="color:#ff0000">Preservation of the saphenous vein</span>'''
* '''<span style="color:#ff0000">Medial: anterolateral border of adductor longus muscle</span>'''
*# '''<span style="color:#ff0000">Elimination of the need to transpose the sartorius muscle</span>'''
* '''<span style="color:#ff0000">Lateral: saphenous vein and femoral vein</span>[https://pubmed.ncbi.nlm.nih.gov/16643509/]'''
* '''<span style="color:#ff0000">Inferior: fossa ovalis (where the saphenous penetrates the fascia lata to drain into the common femoral vein)[https://www.youtube.com/watch?v=5HdhCDdDnP0]</span>'''
*Technique
*'''<span style="color:#ff0000">Floor: pectineus muscle for deep dissection (fascia lata for superficial)</span>'''
**Position: frog-leg
**Note that adductor longus and sartorious are posterior to fascia lata and are therefore not the relevant medial and lateral boundaries for superficial dissection.
** A 10-cm skin incision is made ≈1.5-2 cm below the inguinal crease
*'''Contemporary modified ILND should include the central and superior zones of the inguinal region[https://pubmed.ncbi.nlm.nih.gov/21481617/] and the deep inguinal nodes'''
** Skin flaps are developed in the plane just beneath the Scarpa fascia for a distance of 8 cm superiorly and 6 cm inferiorly.
==== Step by step ====
** The superior dissection is carried to the level of the external oblique fascia with exposure of the spermatic cord. A funiculus of lymphofatty tissue, extending from the base of the penis to the superomedial portion of the lymph node packet, is ligated and divided.
** Dissection commences in a caudad direction with removal of the superficial and deep inguinal nodes
*'''Similar to standard inguinal lymph node dissection with the following adjustments'''
** The saphenous vein is identified and preserved, although a number of branches draining into it will need to be sacrificed.
** '''Incision: 10-cm skin incision is made ≈1.5-2 cm below the inguinal crease extending from just lateral to the femoral artery to the area of the adductor longus muscle[https://pubmed.ncbi.nlm.nih.gov/30730389/][https://pubmed.ncbi.nlm.nih.gov/21481617/]'''
** The nodal packet is dissected caudad to the level of the skin flap dissection, at which point the lymphatics are carefully ligated and the specimen is delivered from the operative field
* The saphenous vein is identified and preserved, although a number of branches draining into it will need to be sacrificed.
** A closed-suction drain is placed, and the incision is closed in standard fashion
*'''Modified dissection should be converted to a radical inguinal lymphadenectomy if positive inguinal lymph nodes are present on frozen section[https://link.springer.com/book/10.1007/978-3-319-60858-7]'''
** Adverse events:
*** Primarily minor
=== Post-operative care ===
**** Seroma or lymphocele (0-26%)
* '''Compression stockings, sequential compression devices, early ambulation, and physical therapy are strongly advised immediately after surgery[https://pubmed.ncbi.nlm.nih.gov/18762945/]'''
**** Lymphorrhea (9-10%)
**Bed rest for 2 or 3 days is only used if myocutaneous or other large skin flap is used.
**** Wound infection and skin necrosis (0-15%)
** Efforts to minimize lymphedema during the initial postoperative period include applying thigh-high elastic wraps or stockings and elevating the foot of the bed.
**Fitted stocking should be after ILND worn when the patient is ambulatory to maintain lower extremity volume. Patients are then assessed at 6 months and given a trial period without the devices. If leg volume increases (assessed by girth measurements) patients are recommended to wear compressive garments on a chronic basis and consulted to lymphedema specialists for massage therapy'''[https://pubmed.ncbi.nlm.nih.gov/18762945/]'''
*Wound site is kept clean and dry
**In obese patients, dry gauze is often placed in the groin crease to prevent excessive moisture and prevent fungal overgrowth.[https://pubmed.ncbi.nlm.nih.gov/18762945/]
* '''Closed-suction rains are removed after when drainage is <30-50 mL/day for consecutive days which typically occurs 3–17 days following surgery<span style="color:#ff0000">[https://link.springer.com/content/pdf/10.1007/978-1-62703-367-1.pdf]</span>'''
**An oral suppressive dose of a cephalosporin can be continued until drains have been removed to assist in sterilizing the port of potential entry for bacteria.[https://pubmed.ncbi.nlm.nih.gov/18762945/]
*Sutures and/or staples are removed on Day 15[https://www.sciencedirect.com/science/article/pii/S1878788623000292]
*'''Complication rates reported to be as high as 50%[https://link.springer.com/book/10.1007/978-3-319-60858-7]'''
**'''Methods to reduce complications (4)'''
**#'''Meticulous usage of clips, instead of electrocautery, to ligate lymphatic channels'''
**#'''Inguinal pressure dressings'''
**#'''Antibiotic regimens'''
**#'''Stockings'''
*'''Strong risk factor for complications is palliative indication for ILND'''[https://pubmed.ncbi.nlm.nih.gov/11912379/ §]
==== Endoscopic and robotic inguinal lymphadenectomy ====
== Minimally Invasive Inguinal Lymphadenectomy ==
* The morbidity of an endoscopic inguinal lymph node dissection is lower than previously reported for open contemporary series with a similar number of nodes being harvested
* The morbidity of an endoscopic inguinal lymph node dissection is lower than previously reported for open contemporary series with a similar number of nodes being harvested
Line 165:
Line 292:
# What part of the penis is drained by the superficial vs. deep lymphatic system?
# What part of the penis is drained by the superficial vs. deep lymphatic system?
# Which lymph nodes do the superficial vs. deep lymphatics of the penis drain to?
#What are the boundaries of dissection in inguinal lymph node dissection?
== Answers ==
== Answers ==
# What part of the penis is drained by the superficial vs. deep lymphatic system?
# What part of the penis is drained by the superficial vs. deep lymphatic system?
# Which lymph nodes do the superficial vs. deep lymphatics of the penis drain to?
#What are the boundaries of dissection in inguinal lymph node dissection?
== References ==
== References ==
* Wein AJ, Kavoussi LR, Partin AW, Peters CA (eds): CAMPBELL-WALSH UROLOGY, ed 11. Philadelphia, Elsevier, 2015, vol 1, chap 39
* Hinman’s Atlas of Urologic Surgery, 4th Edition Joseph A. Smith, Jr., Stuart S. Howards, Glenn M. Preminger, Roger R. Dmochowski
*Wein AJ, Kavoussi LR, Partin AW, Peters CA (eds): CAMPBELL-WALSH UROLOGY, ed 11. Philadelphia, Elsevier, 2015, vol 1, chap 39
*Leone, Andrew, et al. "Contemporary management of patients with penile cancer and lymph node metastasis." ''Nature Reviews Urology'' 14.6 (2017): 335-347.
*Leone, Andrew, et al. "Contemporary management of patients with penile cancer and lymph node metastasis." ''Nature Reviews Urology'' 14.6 (2017): 335-347.
Clinically node-positive disease (palpable on physical exam)
Clinically node-negative disease (not palpable on physical exam) but increased risk for inguinal metastasis based on primary tumor characteristics (pT ≥2, presence of vascular or lymphatic invasion, or grade ≥3).
cN3 (fixed nodal mass) is managed initially with neoadjuvant chemotherapy followed by radical inguinal lymphadenectomy in responders
May be curative when the disease is limited to the inguinal nodes.
Empties into the right and left superficial inguinal nodes
Deep lymphatic system
Drains the glans penis
Empties into the superficial inguinal nodes and the deep inguinal nodes
Primary site of metastatic spread of penile carcinoma occurs via the regional lymphatic system, first to the inguinal lymph node chain and then to the iliac and pelvic lymph nodes.
Penetration of Buck’s fascia or the tunica albuginea by the primary penile tumor allows for dissemination of tumor cells into the lymphatic system
Presence and extent of regional LN metastases is the single most important prognostic factor in determining the long-term survival of patients with penile cancer
If cancer has spread to the pelvic nodes, long-term survival is < 10%
Inguinal metastatic spread can be unilateral or bilateral
Crossover drainage from the right to left groin or vice versa can also occur
Metastatic spread from the inguinal lymph nodes to the contralateral pelvis or from the right to left pelvis has never been reported.
Skip lesions with direct lymphatic drainage from penile tumors to the pelvic lymph nodes has never been reported.
Further spread from the true pelvis to the retroperitoneal lymph nodes is beyond the regional drainage system of the penis and represents systemic metastatic disease
Broad-spectrum antibiotics (e.g. ampicillin/gentamycin or ampicillin/ciprofloxacin)[1][[
In patients with pre-operative cellulitis or infection of the groin region, oral antibiotics (i.e., usually a 1st generation cephalosporin or penicillin) to treat and control this infection prior to surgical management is strongly advised.[2]
If the primary tumor is infected, Inguinal lymphadenectomy is best performed in a staged fashion n order to remove the infected source and provide appropriate antibiotic coverage based upon the clinical circumstances
Oblique incision ≈2-3 cm below and parallel to the inguinal ligament (groin crease)[5]
Lateral end
Radical inguinal lymphadenectomy: line drawn from the anterior superior iliac spine extending inferiorly
Modified inguinal lymphadenectomy: vertical line drawn from above the femoral artery
Medial end
Radical or modified inguinal lymphadenectomy: line drawn from the pubic tubercle extending inferiorly
Special scenario: When the overlying skin is involved with disease secondary to direct tumor invasion or broken down by infection or prior therapy and requires excision, consider an elliptical incision with resection of the involved skin and the subcutaneous tissue[6]
In this setting, the incision may alternatively be extended superiorly from the lateral border of the ellipse and inferiorly from the medial border to make a single S-shaped incision for the iliac and inguinofemoral dissections
Standard radical inguinal lymphadenectomy[edit | edit source]
In the standard radical inguinal lymphadenectomy, both the superficial and deep inguinal lymph nodes are removed
Superior: inguinal ligament/superior boundary of the external oblique aponeurosis and the spermatic cord
Inguinal ligament is the portion of the external oblique aponeurosis which extends between the anterior superior iliac spine and the pubic tubercle as a thick band, folded inward[9]
Medial: anterolateral border of adductor longus muscle
Lateral: sartorious muscle (saphenous vein and femoral vein in modified template)[10]
Inferior: apex of the femoral triangle/fossa ovalis (where the saphenous penetrates the fascia lata)
Floor: pectineus muscle for deep dissection (fascia lata for superficial)
Note that adductor longus and sartorious are posterior to fascia lata and are therefore not the relevant medial and lateral boundaries for superficial dissection.
Externally rotate the hip and flex the knee. Place cushioned support under the flexed knees.
Prepare area with chlorhexidine–alcohol scrub
Preoperative skin preparation with a chlorhexidine–alcohol scrub provided a significantly lower surgical site infection rate at 30 days when compared to a skin prep with a povidone–iodine solution
Drape with exposure of the umbilicus, pubic tubercle, anterior superior iliac spine, and anterior thigh
Use marking pen to denote landmarks and incision.
Landmarks
Anterior superior iliac spine
Pubic tubercle
If middle finger is on pubic symphysis, index finger is on pubic tubercle
Inguinal ligament (line from anterior superior iliac spine to pubic tubercle)
Femoral artery (if palpable, usually located approximately at the midpoint of the inguinal ligament)
Fossa ovalis/saphenous opening (3–4 cm inferior and lateral to the pubic tubercle)
Lateral end of incision is to a line drawn from the anterior superior iliac spine extending inferiorly and the medial end of the incision is to a line drawn from the pubic tubercle extending inferiorly
The boundaries of dissection in a radical inguinal lymphadenectomy are defined by the superior margin of the external ring to the anterior superior iliac spine, laterally from the anterior superior iliac spine extending 20 cm inferiorly and medially to a line drawn from the pubic tubercle 15 cm downward[12]
Develop and raise superior and inferior skin flaps
Use left hand to retract and Metzenbaum scissors/cautery to develop and raise superior and inferior skin flaps below Camper's fascia down to the level of the external oblique aponeurosis to expose the inferior border of the inguinal ligament and spermatic cord.
Important to leave a 6—8 mm thickness of subcutaneous tissue in contact with the skin to avoid necrosis[13]
Care should be taken to preserve the superficial blood supply to the flaps, thus minimizing the risk of postoperative skin necrosis, infection, and wound breakdown
Camper’s fascia can be preserved and left attached to the overlying skin when the superior and inferior skin flaps are fashioned.
Lymphatic drainage of the penis to the groin runs beneath the Camper fascia
Camper's fascia may appear as glistening layer
Superior skin and subcutaneous tissue flap is developed ≈8 cm superiorly[14] towards the inguinal ligament
Fascia lata is continuous with Scarpa fascia superiorly, transitions at inguinal ligament
Majority of the lymph nodes will be found in the central and medial zones[21]
Anatomic lymph groups (5) by location:
Central nodes around the saphenofemoral junction
Superomedial nodes around the superficial external pudendal and superficial epigastric veins
Drain the prepuce of the penis and the scrotum
Inferomedial nodes around the greater saphenous vein
Superolateral nodes around the superficial circumflex vein
Inferolateral nodes around the lateral femoral cutaneous and superficial circumflex veins
In obese patients, it may be easy to overlook the superior medial zone nodal tissue if a prominent suprapubic fat pad is present.
Identify and ligate veins in this area, which can include (see Figure)
Superficial epigastric vein (drains into the greater saphenous vein proximally) at the superior boundary of dissection
Superficial circumflex iliac vein (drains into the greater saphenous vein laterally) at the superior boundary of dissection
External pudendal vein (drains into the greater saphenous vein medially)
Anterior/lateral accessory saphenous vein (drains into the greater saphenous vein laterally)
Superior boundary: dissect the fat and areolar tissues to the level of the external oblique fascia, the external inguinal ring, and the exposure of the spermatic cord
Ligate and divide the first lymphatic packet: a funiculus of lymphofatty tissue, extending from the base of the penis to the superomedial portion of this lymph node packet[22][23]
Then from the iliac bone, then from the inguinal ligament (this should expose the femoral vessels)[24]
Inferior boundary: inferior angle of the inguinofemoral exposure at the apex of the femoral triangle
Lateral boundary: anterior superior iliac spine (circumflex iliac vessels that can be ligated)[25]
Identify the Great saphenous vein at the inferior boundary of the femoral triangle
Great saphenous vein approaches common femoral vein medially
In standard radical inguinal lymphadenectomy, the great saphenous vein and the lateral saphenous vein are divided at the saphenofemoral junction. However, this increases the risk of lower-extremity complications
In modified inguinal lymphadenectomy (see below), the Great saphenous vein is spared.
In patients with minimal metastatic disease, it may be feasible and beneficial to spare the saphenous vein.
Medial boundary: Dissect medially to identify the aponeurosis of the adductor longus muscle of the thigh
Lateral boundary: Dissect laterally to identify the aponeurosis of the sartorius muscle [or up to the circumflex iliac vessels
Deep lymph node dissection
Enter the fascia lata
Overlying the sartorius muscle laterally and medially through the thinner fascia of the adductor longus muscle[26]
Lies 3-4cm below and lateral to the pubic tubercle
Transmits the great saphenous vein and other smaller vessels including the superficial epigastric artery and superficial external pudendal artery, as well as the femoral branch of the genitofemoral nerve[28]
Identify the femoral artery and vein at the apex of the femoral triangle. Use the femoral vessels to guide the dissection along superiorly[29]
The anterior aspects of the femoral vessels are dissected, but the femoral vessels are not skeletonized, and the lateral surface of the femoral artery is not exposed.[30]
This avoids injury to the femoral nerve and the deep femoral artery
The femoral nerve is usually not visible as it runs beneath the iliacus fascia lateral to the femoral artery.
Branches of the femoral nerve can be on the lateral border of the femoral artery, which must be preserved.
Be careful when dissecting over the femoral vessels
Continue dissection superiorly along the anterior surface of the femoral vein and the femoral artery working medially to laterally over the femoral vein and artery up to the inguinal ligament until the femoral canal is reached where continuity to the pelvic dissection is attained to include the deep inguinal nodes.
The femoral canal is located medial to the femoral vein below the inguinal ligament
Superficial cutaneous perforating arteries are ligated as they are encountered on the surface of the femoral artery.
Use both blunt and sharp dissection to resect the deep inguinal nodes.
The deep nodes are typically no more than 3–5 lymph nodes contained within the femoral sheath[31]
The node of Cloquet is the most proximal in the femoral canal and considered the margin between the inguinal and pelvic lymph nodes[32]
Cloquet’s lymph node is removed.
Clip and transect specimen at the level of the femoral canal
Send intraoperative frozen section of lymph node packet
Intraoperative frozen section has been shown to have diagnostic value in determining the need to proceed to a radical dissection[33]
It may be time-saving to proceed to the contralateral dissection while awaiting frozen section results.
Apply sartorius flap, if needed, forcoverage over the femoral vessels and nerves
If a deep dissection, the sartorius muscle can be transposed or rolled 180 degrees medially by releasing its attachments from the anterior superior iliac spine, providing myocutaneous coverage over the femoral vessels and nerves
The sartorius flap is sutured to the inguinal ligament superiorly with interrupted 2-0 Vicryl sutures, and its margins are sutured to the muscles of the thigh immediately adjacent to the femoral vessels[34]
Closure
Irrigate the wound
Irrigate aggressively with water or saline using a bulb syringe to remove small clots and uncover a potential bleeding source.[35]
Insert multiperforated closed-suction drains (10 or 15 French)
Place drains under the subcutaneous tissue in the dissected area along the femoral vascular axis[36] and bring the drains out inferiorly, to prevent lymphocele formation.
Primary closure of the inguinofemoral dissection is usually possible with minimal or no further mobilization of the excision margins.
When circumstances demand a large area of inguinal soft tissue sacrifice, primary closure may be obtained by scrotal skin rotation flaps an abdominal wall advancement flap or a myocutaneous flap based on the rectus abdominis or tensor fasciae latae for more extensive defects.
Suture skin flips to the surface of the exposed musculature to decrease dead space.
This can minimize the risk of a postoperative fluid collection (i.e., seroma) that may serve as a potential source for infection.
Reapproximate subcutaneous tissues with 2-0 Vicryl
Reapproximate skin with 3-0 non-absorbable suture or skin staples[37]
Clinically node-negative disease (not palpable on physical exam) but increased risk for inguinal metastasis based on primary tumor characteristics (pT ≥2, presence of vascular or lymphatic invasion, or grade ≥3).
Superior: inguinal ligament/superior boundary of the external oblique aponeurosis and the spermatic cord
Inguinal ligament is the portion of the external oblique aponeurosis which extends between the anterior superior iliac spine and the pubic tubercle as a thick band, folded inward[46]
Medial: anterolateral border of adductor longus muscle
Inferior: fossa ovalis (where the saphenous penetrates the fascia lata to drain into the common femoral vein)[48]
Floor: pectineus muscle for deep dissection (fascia lata for superficial)
Note that adductor longus and sartorious are posterior to fascia lata and are therefore not the relevant medial and lateral boundaries for superficial dissection.
Contemporary modified ILND should include the central and superior zones of the inguinal region[49] and the deep inguinal nodes
Similar to standard inguinal lymph node dissection with the following adjustments
Incision: 10-cm skin incision is made ≈1.5-2 cm below the inguinal crease extending from just lateral to the femoral artery to the area of the adductor longus muscle[50][51]
The saphenous vein is identified and preserved, although a number of branches draining into it will need to be sacrificed.
Modified dissection should be converted to a radical inguinal lymphadenectomy if positive inguinal lymph nodes are present on frozen section[52]
Compression stockings, sequential compression devices, early ambulation, and physical therapy are strongly advised immediately after surgery[53]
Bed rest for 2 or 3 days is only used if myocutaneous or other large skin flap is used.
Efforts to minimize lymphedema during the initial postoperative period include applying thigh-high elastic wraps or stockings and elevating the foot of the bed.
Fitted stocking should be after ILND worn when the patient is ambulatory to maintain lower extremity volume. Patients are then assessed at 6 months and given a trial period without the devices. If leg volume increases (assessed by girth measurements) patients are recommended to wear compressive garments on a chronic basis and consulted to lymphedema specialists for massage therapy[54]
Wound site is kept clean and dry
In obese patients, dry gauze is often placed in the groin crease to prevent excessive moisture and prevent fungal overgrowth.[55]
Closed-suction rains are removed after when drainage is <30-50 mL/day for consecutive days which typically occurs 3–17 days following surgery[56]
An oral suppressive dose of a cephalosporin can be continued until drains have been removed to assist in sterilizing the port of potential entry for bacteria.[57]
The morbidity of an endoscopic inguinal lymph node dissection is lower than previously reported for open contemporary series with a similar number of nodes being harvested



{kind=link}
{kind=link}
{kind=link}