Functional: Surgery for Male SUI
See 2019 AUA Incontinence after Prostate Therapy Guideline Notes
Causes of Male SUI[edit | edit source]
- Stress urinary incontinence (SUI) develops only in men with concomitant (2):
- Internal sphincter impairment
- External sphincter impairment
- Causes of internal sphincter impairment (5):
- Pelvic surgery
- Bladder neck injury
- Specific sympathetic neuropathic dysfunction
- Embryologic disruption
- Causes of external sphincter impairment (5):
- Radical prostatectomy (most common cause)
- TURP
- Incontinence after TURP may reflect persistent bladder overactivity but rarely results from damage to the external sphincter during resection
- In a large Veterans Study, the rate of de novo UI after TURP was no different from that in the watchful waiting group
- Pelvic fracture urethral injuries
- Myelopathy (traumatic and acquired)
- Congenital disorders such as spinal dysraphism, sacral agenesis, and the exstrophy/epispadias complex
Diagnosis and Evaluation[edit | edit source]
UrologySchool.com Summary[edit | edit source]
- Recommended
- History and Physical Exam, including degree of bother
- Labs
- Urinalysis +/- culture
- Other
- Appropriate diagnostic modalities to categorize type and severity of incontinence (e.g. voiding diary, pad weights)
- Optional
- Post-void residual
History and Physical Exam[edit | edit source]
- History
- Characterize incontinence
- Type of incontinence
- Treatment for SUI (caused by sphincteric insufficiency) vs. urgency incontinence (caused by bladder dysfunction) are different.
- In cases of mixed incontinence, determine which component is more prevalent and bothersome (stress or activity related versus urgency related)
- Increases in abdominal pressure such as that caused by straining, walking, cough, and exercise are suggestive of SUI
- The sudden compelling desire to void that is difficult to defer and results in leakage indicates urgency incontinence.
- Presence of incontinence while asleep as well as nocturia are also important to note, because this may indicate urgency urinary incontinence or severe SUI.
- In cases of mixed incontinence, determine which component is more prevalent and bothersome (stress or activity related versus urgency related)
- Differentiation between stress and urge UI can be aided by the voiding diary and pad test
- Treatment for SUI (caused by sphincteric insufficiency) vs. urgency incontinence (caused by bladder dysfunction) are different.
- Progression or resolution of incontinence over time, exacerbating factors
- Severity of incontinence (i.e. volume lost over time)
- Can be determined by history, or more objectively, by pad testing
- In the case of sphincteric insufficiency, some treatments (e.g., male slings), clearly have inferior results in severe incontinence.
- Degree of bother
- Type of incontinence
- Previous surgical procedures
- Symptoms of neurologic disease
- Characterize incontinence
- Physical exam
- Abdomen, back, genitalia, perineum, rectum, and neurologic system
- Scrotal exam
- May detect pathologic processes that can influence pump placement such as hydrocele, hernias, and scrotal masses.
- If inguinal hernia identified and contralateral pressure-regulating balloon (PRB) placement is not possible, concomitant hernia repair is advisable.
- May detect pathologic processes that can influence pump placement such as hydrocele, hernias, and scrotal masses.
- Previous surgical incisions should be noted when planning AUS pressure-reservoir balloon placement
Labs[edit | edit source]
- Urinalysis +/- culture are required before surgical correction of male UI
Other[edit | edit source]
- Cystoscopy
- Should be performed to assess for urethral and bladder pathology that may affect outcomes of surgery★
- Patients with symptomatic vesicourethral anastomotic stenosis or bladder neck contracture should be treated prior to surgery for incontinence after prostate therapy
- Unrecognized urethral pathologic processes can significantly complicate all surgical approaches
- Patients with symptomatic vesicourethral anastomotic stenosis or bladder neck contracture should be treated prior to surgery for incontinence after prostate therapy
- Should be performed to assess for urethral and bladder pathology that may affect outcomes of surgery★
- Urodynamics (UDS) may be performed★
- UDS are not required before surgical intervention for incontinence after prostate therapy unless the clinician is in doubt of the diagnosis or it is felt that patient counseling will be affected.
- During UDS, it is important that the catheter be removed and stress testing repeated in patients with suspected SUI who do not demonstrate stress incontinence with a catheter in place
- Up to 35% of males with post-prostatectomy SUI will not demonstrate SUI with a catheter in place. This may be due to some scarring at the site of the anastomosis. In such cases, even a small catheter can occlude the urethra and prevent stress leakage.
- During UDS, it is important that the catheter be removed and stress testing repeated in patients with suspected SUI who do not demonstrate stress incontinence with a catheter in place
- Intrinsic sphincteric dysfunction will be identified in almost all cases.
- In 2012, the American Urological Association (AUA) released guidelines on the use of urodynamics in the clinical evaluation of the patient with voiding dysfunction.
- Specific recommendations for the patient with SUI include at minimum that: surgeons considering invasive therapy in patients with SUI should assess the PVR.
- Furthermore, clinicians may perform multichannel urodynamics in patients with both symptoms and physical findings of stress incontinence who are considering invasive, potentially morbid or irreversible treatments, which include placement of the male sling or AUS.
- Detrusor hypocontractility may indicate the need for AUS instead of sling if adequate detrusor function does not exist to overcome the fixed resistance of a compressive sling
- Reduced bladder compliance is concerning because prolonged storage at high pressures may lead to deteriorating renal function.
- UDS are not required before surgical intervention for incontinence after prostate therapy unless the clinician is in doubt of the diagnosis or it is felt that patient counseling will be affected.
Management[edit | edit source]
- Patients with urgency urinary incontinence or urgency predominant mixed urinary incontinence should be offered treatment options per the AUA Overactive Bladder Guidelines
Options[edit | edit source]
- Non-surgical (6):
- Pelvic floor muscle exercises (PFME)/Pelvic floor muscle training (PFMT)
- Absorbent pads
- Penile compression devices such as Dribble-Stop
- Condom catheter
- Urethral catheter
- Duloxetine (a serotonin norepinephrine reuptake inhibitor)
- All except duloxetine are described in 2019 AUA Guidelines on Incontinence After Prostate Therapy
- Surgical (5):
- Transurethral bulking agents
- Adjustable balloon devices (ProACT)
- Bulbar urethral sling
- Artificial Urinary Sphincter (AUS)
- Bladder neck closure with diversion
Non-surgical[edit | edit source]
Pelvic floor muscle exercises (PFME)/Pelvic floor muscle training (PFMT)[edit | edit source]
- Should be offered to all patients★
- Advantages:
- Safe treatment with minimal side-effects
- Provides patients with an opportunity to participate in their health outcomes.
- Disadvantages:
- Time and effort required
- Cost of repeated visits for PFMT
- Males with SUI should initially be treated with pelvic floor muscle training for at least 3 months
- After radical prostatectomy, it is recommended that no surgical treatment be considered until at least 6-12 months subsequently as some patients will continue to improve.
- Progressive improvement in urinary control has been reported to occur for as long as 2 years after surgery
Penile Compression Devices[edit | edit source]
- Should not be left on the phallus overnight due to the risks of constant pressure
- Not suitable for patients with (4):★
- Memory deficits
- Poor manual dexterity
- Impaired sensation
- Significant component of OAB
Urethral catheter[edit | edit source]
- Last resort in a patient who is unsuitable for alternative management
- Suprapubic catheter drainage is not a solution for the patient with severe intrinsic sphincter deficiency, as urethral leakage will persist
Surgical[edit | edit source]
Timing[edit | edit source]
- If there is no improvement at 6 months despite conservative therapy and the patient has bothersome IPT, (i.e. patient does not want to wait until 12 month time point) surgery may be considered for early treatment
- While almost all patients have reached their maximum improvement by 12 months, most patients with severe SUI will show no significant improvement after 6 months and may be candidates for early intervention
- Otherwise, treatment should be offered to patients with persistent bothersome SUI at 12 months.
- Conversely, treatment should be offered with caution in some patients who continue to display symptom improvement at 12 months
Contraindications[edit | edit source]
- 2019 AUA Guidelines on Incontinence After Prostate Therapy: It is not known if poor bladder compliance and an uncorrected storage pressure are absolute contraindications to SUI surgery in IPT patients. However, these patients should be carefully followed to avoid upper tract decompensation.
- Relative
- Urinary tract abnormalities that require future transurethral management, such as
- Bladder cancer
- Refractory vesicourethral anastomotic strictures
- In such cases, an AUS or sling procedure could impair transurethral access and repeated instrumentation may put the devices at risk for infection or erosion.
- Urinary tract abnormalities that require future transurethral management, such as
- Detrusor overactivity, if present, is not a contraindication to the treatment for sphincteric incontinence but requires realistic counseling regarding the likelihood of successful outcome
- Factors to consider include the severity of UI and associated bother; patient characteristics, including BMI, prior surgical procedures, adjuvant radiation therapy, bladder function, and cystoscopic findings; manual dexterity and cognitive function; efficacy of the various implants; long-term risk for complications and reoperation; and patient preference
Options (5):[edit | edit source]
- Transurethral bulking agents
- Adjustable balloon devices (ProACT)
- Bulbar urethral sling
- Artificial Urinary Sphincter (AUS)
- Bladder neck closure with diversion
Transurethral bulking agents[edit | edit source]
- Advantage
- Least invasive technique
- Disadvantage
- Least effective surgical technique
- Cure is rare
- Least effective surgical technique
- Indication
- Consider in patients who are unable to tolerate or refuse more invasive surgical therapy
- Limited role after prostatectomy given the severity of incontinence and post-surgical scarring in the vesicourethral region
- A trial of bulking agent may be appropriate in men with neurogenic SUI
- Consider in patients who are unable to tolerate or refuse more invasive surgical therapy
Adjustable balloon devices (ProACT)[edit | edit source]
- Disadvantages
- Increased incidence of intraoperative complications and need for explanation within the first 2 years compared to the male sling and AUS
- Indication
- Consider for mild SUI
Bulbar Urethral Sling[edit | edit source]
- Indication
- Consider for mild to moderate SUI
- Mild-to-moderate incontinence defined as a 24-hour pad weight < 150 g for mild UI and < 400 g for moderate UI
- Poor efficacy in comparison to an AUS in patients with severe incontinence.
- Alternatives for those who refuse AUS from fear of infection, erosion, or mechanical failure, as well as those with limited physical or cognitive capacity
- Consider for mild to moderate SUI
- Contraindications (3):
- Radiation
- Urethral erosion
- Severe gravitational urinary incontinence
- Types (3)
- InVance (AMS): mesh placed outside the bulbospongiosus muscle and anchored to the pubic rami
- No longer available in the US
- Mechanism of continence thought to be from compression of urethra
- AdVance (AMS): transobturator fixation of mesh
- Mechanism of continence thought to be from enhanced rhabdosphincter function without significant compression; designed to reposition and lengthen the membranous urethra
- See Figure
- Virtue (Coloplast): combined prepubic and transobturator sling
- Four-armed mesh device (quadratic fixation) that provides a long segment of urethral compression against the urogenital diaphragm and a separate elevation component because of the prepubic and transobturator arms, respectively
- Limited data on efficacy and durability
- InVance (AMS): mesh placed outside the bulbospongiosus muscle and anchored to the pubic rami
- After urethral disruption due to pelvic fracture, neither the InVance or the AdVance slings are likely to reliably provide effective elevation, elongation, or compression because of distortion of the bony pelvic anatomy and high likelihood of rhabdosphincter damage
- Technique
- Determining the appropriate tension of the sling is the most critical portion of the operation
- Adverse events (generally low complication rate):
- Urinary retention
- Typically resolves within 1 week
- Pelvic and perineal pain and paresthesia
- Typically resolves within 12 weeks
- Anchoring complications from bone anchors
- Erosion or infection
- Both are exceedingly rare.
- If a male sling is thought to be infected or documented to be eroded on cystoscopy, the management is similar to management of an infected or eroded AUS (see below)
- Both are exceedingly rare.
- Urinary retention
Artificial Urinary Sphincter (AUS)[edit | edit source]
- Gold standard (AMS 800) for the treatment of SUI in males
- Advantages
- Long-term durability
- Revision rates:
- 2 years: 16%
- 5 years: 28%
- Revision rates:
- Effective across the spectrum of moderate and severe degrees of urinary loss
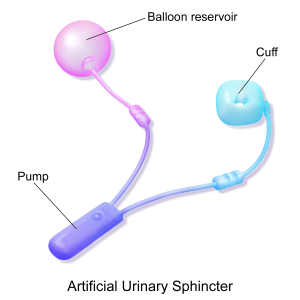
3 parts of the Artificial Urinary Sphincter: Cuff, Balloon reservoir, Pump. Source: Wikipedia
- Long-term durability
- Device consists of (3)[1]
- Control pump
- Pressure-regulating balloon (PRB)
- Fluid-filled cuff placed around the bladder neck or bulbar urethra, of varying sizes
- Provides a 2-cm zone of circumferential compression.
- The degree of compression is determined by the compliance of the pressure-regulating balloon (PRB), with the pressure selected based on patient tissue characteristics and location of the cuff.
- The standard PRB for bulbar AUS is 61-70 cm H2O and balances the need for occlusion with the risk for erosion. Lower pressures provide reduced continence rates but may be advisable if risk for erosion is considered excessive
- The degree of compression is determined by the compliance of the pressure-regulating balloon (PRB), with the pressure selected based on patient tissue characteristics and location of the cuff.
- Provides a 2-cm zone of circumferential compression.

{kind=link}

{kind=link}

{kind=link}
Indications[edit | edit source]
- Consider for mild to severe SUI
- Preferred in patients with prior (3):
- Radiation
- Improved outcomes compared to male slings or adjustable balloons for treatment of patients with SUI after primary, adjuvant, or salvage radiotherapy
- Complication rates are higher
- Urethral reconstruction
- Urethral strictures of the anterior urethra and urethral stenosis of the posterior urethra can arise after RP, RT, or treatment for IPT. Urethral reconstructive surgery is often used to treat narrowing in the urethra.
- Male slings will not be effective given post-surgical changes related to most types of urethral reconstruction in the posterior and anterior urethra
- Complications rates are higher
- Depending on the technique employed (urethra transecting or not) the blood supply to the urethra may be diminished and potentially decrease the life span of an AUS.
- Vesicourethral anastomotic stenosis or bladder neck contracture
- Decreased success rates when undergoing male slings
- Radiation
Contraindications§[edit | edit source]
- Absolute (6):
- Lack of physical or mental dexterity to manipulate the pump
- Repetitive urinary tract infections
- Urethral diverticula at the expected implant site/Poor urethral tissue integrity
- Complex, unstable, or recurrent urethral stricture diseases
- Small capacity and/or non-compliant bladder prior to definitive treatment
- Active infection at surgical site
- Relative (4):
- High-grade vesicoureteric reflux
- Recurrent intravesical or intraurethral diseases such as stones or tumors that are expected to require repeat transurethral instrumentation
- Bulbar urethral placement of an AUS will not allow appropriate instrumentation and transurethral resection in patients with recurrent bladder tumors; in these patients, a male sling is preferred
- A male sling will allow passage of a 24-Fr resectoscope
- Bulbar urethral placement of an AUS will not allow appropriate instrumentation and transurethral resection in patients with recurrent bladder tumors; in these patients, a male sling is preferred
- Bladder neck contracture prior to treatment
- Detrusor overactivity
- Radiotherapy is not considered to be a contraindication for placement of the AUS in males§
Technique[edit | edit source]
- Cuff is most commonly placed around bulbar urethra via a perineal incision. The aim is to place the cuff as proximal on the bulbar urethra as possible, proximal to the convergence of the corporeal bodies
- Single cuff perineal approach is preferred, superior outcomes compared to transverse scrotal incision★
- Summary of Steps
- After incision of the skin, Colles fascia, and bulbospongiosus muscle, the Buck fascia is incised as it reflects off the bulbar urethra onto the diverging corporeal bodies.
- Create a 2-cm wide tunnel under direct vision using sharp dissection, dorsal to the Buck fascia over the roof of the urethra.
- Pass a right-angle clamp through this tunnel.
- Measure the circumference of the urethra around the corpus spongiosum to guide selection of cuff size, most commonly 4 or 4.5 cm.
- Pass the tubing from the AUS cuff through the overlying bulbospongiosus muscle into the deep perineal space beneath the Colles fascia.
- Place the pressure-regulating balloon
- May be achieved through a scrotal, perineal, or abdominal incision, depending on prior surgical incisions, body habitus, and surgeon preference.
- Contraindications to the scrotal/perineal approach:
- Mesh hernia repairs
- Radical cystectomy and other extensive abdominal surgery
- In such cases, the abdominal approach reduces the risk for bladder or intestinal injury
- Contraindications to the scrotal/perineal approach:
- May be achieved through a scrotal, perineal, or abdominal incision, depending on prior surgical incisions, body habitus, and surgeon preference.
- Place the pump assembly into the anterior scrotum from the inguinal, scrotal, or perineal incision.
- After completing the connections, the device is cycled several times through the activation and deactivation states.
- Verify adequate coaptation of the urethra via urethroscopy.
- The closed cuff should cause slight blanching of the urethral tissue, indicating adequate urethral coaptation, filling, and connection of the device.
- Bladder neck AUS
- Remains an optional, although more invasive, method of cuff placement in men with sphincteric UI in whom the prostate is without external surgical or traumatic disruption.
- Thus, for cases of myelomeningocele and other neuropathic disorders, it should be considered as an alternative to bulbar AUS.
- Contraindicated after radical prostatectomy
- Advantages include lower likelihood of erosion and cuff atrophy
- Requires higher PRB pressures to ensure coaptation
- Remains an optional, although more invasive, method of cuff placement in men with sphincteric UI in whom the prostate is without external surgical or traumatic disruption.
- Postoperative deactivation of the cuff for 4-6 weeks is essential for proper healing without erosion.
Adverse Events[edit | edit source]
- Intra-operative
- Urethral injury
- Urethral injury during any implant surgery places the patient at risk for device infection due to the presence of colonizing bacteria in the urethra.
- If identified during implantation, the defect should be repaired, procedure should be abandoned and subsequent implantation should be delayed★
- The risk of devastating device infection outweighs any benefit and thus the procedure should be aborted.
- The defect should be repaired and a catheter inserted for 7 days
- Urethral injury
- Early Post-operative
- Infection
- Device infection occurs in <1-5% of cases
- Skin pathogens (staphylococcus epidermidis (most common) and staphylococcus aureus) are the most commonly cultured organisms
- Diagnosis and Evaluation
- Presents with pain at the site of the AUS/scrotal pain, fever, scrotal warmth, erythema, edema, or skin changes, or frank purulence
- Management
- Urgent AUS explantation★
- Implant infections are not amenable to antibiotic therapy
- Traditional management includes device removal followed by a waiting period of several months with delayed reimplantation.
- AUS should not be reimplanted until at least 3 months to allow the infection to clear and inflammation to subside.★
- Urgent AUS explantation★
- Urinary Retention
- Diagnosis and Evaluation
- Rule out inadvertent cuff activation
- Management
- In the immediate postoperative period, should be managed by with a small (10 or 12 Fr) catheter for 24-48 hours. Cuff deactivation must be confirmed before catheterization.
- Instructions to deactivate AUS (pdf) (video)
- If the patient fails a voiding trial at 48 hours, suprapubic cystostomy drainage is recommended to reduce the risk for urethral erosion
- Retention persisting beyond several weeks implies undersizing of the cuff; in such cases, reoperation and cuff replacement may be required. Correlation with preoperative urodynamic findings is advised in such cases.
- In the immediate postoperative period, should be managed by with a small (10 or 12 Fr) catheter for 24-48 hours. Cuff deactivation must be confirmed before catheterization.
- Diagnosis and Evaluation
- Infection
- Late Post-operative
- Persistent leakage
- Cuff erosion
- Occurs in up to 5% of AUS implantations
- Introduction of narrow back modification of AUS has reduced the risk of erosion
- Can be due to unrecognized urethral injury at the time of initial surgery or more likely due to subsequent instrumentation of the urethra including catheterization.
- Risk factors
- Campbell’s: radiation therapy, prior erosions with the need for removal of the device, prolonged catheterization and instrumentation, hypertension and other comorbidities
- No increased risk of erosion with prior transobturator sling
- SASP 2016: radiation therapy, prior erosions or infection in a previous AUS, a prior urethroplasty, multiple endoscopic treatments for bladder neck contracture or urethral stricture, or prior urethral stent placement. There is also a much lower but still significant increased risk of erosion with a prolonged postoperative catheterization interval (> 48 hours), or use of either a 3.5 cm or transcorporal cuff compared to a standard 4 cm cuff.
- No increased risk of erosion with increasing age, proximal or distal bulbar urethral placement of the AUS, or prior radical prostatectomy
- Campbell’s: radiation therapy, prior erosions with the need for removal of the device, prolonged catheterization and instrumentation, hypertension and other comorbidities
- Management
- AUS explant with the urethral catheter left in place for a few weeks to allow the urethral defect to heal★
- Immediate removal of all the components of the AUS is imperative because they are assumed to be infected.
- AUS should not be re-implanted until at least 3 months and urethral healing is confirmed by urethrography
- AUS explant with the urethral catheter left in place for a few weeks to allow the urethral defect to heal★
- Occurs in up to 5% of AUS implantations
- Urethral atrophy
- Results from the chronic compression of the spongy tissue under the occlusive cuff
- Most common cause of gradual return of incontinence and revision of the AUS
- Management
- Options:
- Cuff downsizing
- Movement of the cuff to a more proximal or distal location where the urethra may be thicker
- Placement of a second cuff in tandem
- Options:
- Mechanical failure
- 7-10-year device life for the AUS
- Rate of device failure increases with time, with failure rates of
- ≈24% at 5 years
- ≈ 50% at 10 years
- Rate of device failure increases with time, with failure rates of
- Causes
- Failure in any of the 3 parts (cuff, balloon reservoir, or pump), the tubing, or connections suffer a micro-perforation with loss of fluid
- Management
- An AUS might need to be replaced over time due to persistent or recurrent incontinence generally due to:
- Urethral atrophy
- Improper cuff sizing
- Partial fluid loss
- In the absence of infection or erosion, replacement of an isolated malfunctioning component may be feasible if the revision occurs within 3 years of implantation.
- However, a slow leak from the PRB may be difficult to diagnose intraoperatively, and, if in doubt, total device replacement is prudent.
- Devices older than 3 years old should be replaced in entirety.
- An AUS might need to be replaced over time due to persistent or recurrent incontinence generally due to:
- 7-10-year device life for the AUS
- Urinary Retention
- Late-onset urinary retention mandates endoscopic and urodynamic evaluation to rule out:
- Proximal urethral obstruction
- Erosion
- Detrusor failure
- Late-onset urinary retention mandates endoscopic and urodynamic evaluation to rule out:
Bladder neck closure or diversion[edit | edit source]
- Can be considered in appropriately motivated and counseled patients who are unable to obtain adequate long-term quality of life
- If bladder preservation is feasible, conversion to a Mitrofanoff (e.g. Appendix, Monti), incontinent ileovesicostomy, or suprapubic tube with bladder neck closure may confer an improved QoL.
- In the event of the “hostile” bladder, cystectomy in combination with either an ileal conduit or continent catheterizable pouch would best manage incontinence while protecting the upper tracts.
- May be required if inadequate tissue integrity at the bladder neck or urethra to accommodate a sling or AUS
Special Situations[edit | edit source]
Persistent Incontinence after Surgery (AUS or sling)[edit | edit source]
- Causes
- Inadvertent deactivation
- Insufficient urethral compression (oversizing of cuff)
- Cuff erosion
- Bladder storage failure
- Mechanical failure with fluid loss
- Plugged delay-fill resistor
- Kinked tubing
- Timing
- After AUS insertion,
- A slow onset of incontinence suggests atrophy
- The sudden recurrence of incontinence indicates
- Mechanical failure
- Fluid leak
- Erosion of the device
- After AUS insertion,
- Inadvertent deactivation
- Active cycling of the device excludes inadvertent deactivation.
- If the pump is deactivated with inadequate fluid to cycle, passive filling can be achieved by squeezing the pump on its lateral edges or by pushing on the pump with a cotton-tipped applicator opposite the deactivation button.
- Active cycling of the device excludes inadvertent deactivation.
- Mechanical failure with fluid loss
- Plain radiography (for contrast-filled systems) or ultrasonography (for saline-filled systems) of the pressure-reservoir balloon during cycling can help differentiate fluid loss from cuff atrophy.
- If the pressure-reservoir balloon size changes with cycling and refills passively, mechanical failure is less likely and thus suggests cuff atrophy
- Plain radiography (for contrast-filled systems) or ultrasonography (for saline-filled systems) of the pressure-reservoir balloon during cycling can help differentiate fluid loss from cuff atrophy.
- Cuff erosion
- Cystoscopy, in addition to excluding erosion, can be used to visualize the cuff during cycling and give insight into the likelihood of atrophy.
- Bladder storage failure
- Urodynamics should be performed when bladder storage failure is suspected
- The best indicators for patients who may develop overactive bladder after treatment of their outlet for sphincteric incontinence include (2):
- Bladder capacity < 200 mL on urodynamics or diary
- Presence of symptomatic overactive bladder before surgical treatment for the incontinence
- Patients with prior radiation therapy may develop urgency and frequency at a later time, but this is not a significant risk factor before proceeding with outlet procedures such as male slings or AUS.
- Leak-point pressure and prior procedures do not indicate a risk for development of overactive bladder.
- The best indicators for patients who may develop overactive bladder after treatment of their outlet for sphincteric incontinence include (2):
- Urodynamics should be performed when bladder storage failure is suspected
- Revision surgery for non-mechanical causes may require (3):
- Tandem cuff
- Modified cuff placement using 3.5-cm cuff
- Transcorporeal placement
- When the cause of persistent UI is incomplete urethral occlusion, the addition of a second tandem cuff around the bulbar urethra can yield satisfactory continence.
- Connection to the existing device requires division of the existing cuff tubing and use of a metal Y connector. An additional 3 mL of fluid must be added to the system.
- However, in a relatively young patient, the cuff should be downsized rather than placing a second cuff to avoid using additional locations on the bulbar urethra, which will be necessary for future device replacements over time.
Urethral stricture[edit | edit source]
- The safest approach for an initial stricture would be laser incision through a smaller caliber endoscope such as a ureteroscope.
- Although exploration of the AUS cuff with uncoupling of the cuff will allow safe endoscopic management of strictures and tumors with resectoscopes, this should be reserved for cases not amenable to simple laser incision with small caliber and scopes.
- Antegrade incision is feasible but offers less control than the retrograde approach.
- Open surgical reconstruction should be reserved for refractory cases.
Climacturia[edit | edit source]
- In a patient with bothersome climacturia, treatment may be offered.
- As with post-prostatectomy SUI, for those with sexual arousal incontinence or climacturia, conservative management (emptying the bladder prior to sex, use of condoms to catch the urine, and PFME) should be the initial treatment
- Imipramine, a tricyclic antidepressant, has been used, but this medication is generally contraindicated in men age > 65 due to the risk of somnolence, falling down, and changes in cognition.
- Both the AUS and the trans-obturator male sling, when implanted for SUI, are associated with high rates of improvement in climacturia
Concomitant IPT and erectile dysfunction[edit | edit source]
- In patients with concomitant IPT and erectile dysfunction, a concomitant or staged procedure may be offered.
Long-term results of AUS and slings[edit | edit source]
- On average 76% of AUS patients were dry (0-1 pad per day)
- Success rates for revision surgery compare favorably with initial surgery, although infection and erosion rates are higher
- Poorer prognosis for patients having undergone prior adjuvant radiotherapy
Questions[edit | edit source]
- What are the contraindications to surgery for male SUI? Specifically, AUS? Sling?
- What are some differences between the InVance and AdVance sling?
- What is the typical pressure in the pressure regulating balloon?
- What are contraindications to scrotal/perineal pump placement?
- Describe the management of urinary retention following insertion of AUS
- What is the most common pathogen involved in AUS infections?
- What are risk factors for AUS erostion?
- List causes of persistent incontinence following insertion of AUS
- What is the most common cause of AUS revision surgery
Answers[edit | edit source]
- What are the contraindications to surgery for male SUI? Specifically, AUS? Sling?
- What are some differences between the InVance and AdVance sling?
- What is the typical pressure in the pressure regulating balloon?
- What are contraindications to scrotal/perineal pump placement?
- Describe the management of urinary retention following insertion of AUS
- What is the most common pathogen involved in AUS infections?
- What are risk factors for AUS erostion?
- List causes of persistent incontinence following insertion of AUS
- Inadvertent deactivation
- Insufficient urethral compression (oversizing of cuff)
- Cuff erosion
- Bladder storage failure
- Mechanical failure with fluid loss
- Plugged delay-fill resistor
- Kinked tubing
- What is the most common cause of AUS revision surgery
- Urethral atrophy
References[edit | edit source]
- Wein AJ, Kavoussi LR, Partin AW, Peters CA (eds): CAMPBELL-WALSH UROLOGY, ed 11. Philadelphia, Elsevier, 2015, chap 91
- Sandhu, Jaspreet S., et al. "Incontinence after prostate treatment: AUA/SUFU guideline." The Journal of urology 202.2 (2019): 369-378.