Open Kidney Surgery
Jump to navigation
Jump to search
Videos[edit | edit source]
Pre-operative evaluation[edit | edit source]
- History and Physical Exam
- History
- For cigarette smokers planned for surgery, if time permits, a 4- to 6-week preoperative smoking cessation program has been shown to reduce postoperative complications.
- History
- Labs
- All patients (3):
- Urinalysis +/- urine culture
- Serum creatinine
- Hemoglobin
- Patients with GFR <60 mL/min or significant proteinuria are at increased risk of requiring dialysis; consider nephrology referral
- Urine culture should be obtained if urinalysis is suggestive of infection; any active UTI should be treated preoperatively
- If locally advanced or metastatic disease, add (2):
- Liver function tests (screen for hepatic dysfunction (Stauffer syndrome)
- Coagulation profile (screen for associated coagulopathy)
- All patients (3):
Pre-operative preparation[edit | edit source]
- Mechanical bowel preparation
- Not indicated for routine open renal surgery
- Indications for mechanical bowel preparation in open renal surgery (2):
- Concern about intestinal involvement of a pathologic process
- Iatrogenic intestinal trauma is likely because of multiple prior abdominal surgeries, with likely requirement of extensive lysis of adhesions.
- Venous thromboembolism prophylaxis
- 2008 AUA best practice statement: intermittent pneumatic compression is recommended in patients undergoing open procedures; consider addition of pharmacologic prophylaxis[1]
- Pre-operative antibiotics
- 2019 AUA guidelines: single dose cefazolin or TMP-SMX are recommended in all cases involving controlled entry into urinary tract (e.g. renal surgery, nephrectomy, partial or otherwise)[2]
- CUA guidelines: do not recommend for renal surgery without involvement of collecting system
- Campbell’s 11th edition: A single dose of cefazolin or clindamycin for patients undergoing renal surgery with negative urine culture is prescribed.
- Renal artery embolization prior to nephrectomy
- Relative indications (2):
- Aid in surgical dissection of large renal tumors
- Palliation of inoperable renal tumors in order to control bleeding for large locally advanced renal tumors.
- Potential benefits (5):
- Shrinkage of an arterialized tumor thrombus to ease surgical removal
- Reduced blood loss
- Facilitation of dissection as a result of tissue plane edema
- Modulation of immune response
- Ability to ligate the renal vein before the renal artery
- Potential risks:
- Post-infarction syndrome, which includes flank pain, nausea, and fever
- Occurs in ≈75% of patients
- In some retrospective series embolization is associated with high blood loss, possibly due to the increased edema associated with the infarcted renal tissue
- Post-infarction syndrome, which includes flank pain, nausea, and fever
- Not utilized by all surgeons because potential risks may outweigh benefit
- Relative indications (2):
Anatomic considerations[edit | edit source]
- Review anatomy for
- Critical landmark structures for kidney surgery
- Right (4):
- Liver
- Duodenum
- Ascending colon
- Inferior vena cava
- Left (4):
- Spleen
- Tail of the pancreas
- Descending colon
- Aorta
- Right (4):
- Abdominal and Chest Wall
- Intercostal space is the anatomic space between two ribs. Since there are 12 ribs on each side, there are 11 intercostal spaces, each numbered for the rib superior to it
- Intercostal nerves emerge from below the costal margin and run between the layers of the internal oblique and transversus abdominis muscles
- Pleural cavity
- The inferior limit of the pleural cavity may lie anywhere between the 10th and 12th ribs.
- Access through the 10th or 11th intercostal space (above the 11th or 12th rib) requires careful mobilization of the lower edge of the pleura to avoid entering it
- Access through the 9th intercostal space (above the 10th rib) inevitably requires entry into the pleural cavity
- The inferior limit of the pleural cavity may lie anywhere between the 10th and 12th ribs.
- Rectus abdominis
- Blood supply
- Upper rectus muscle is supplied by the superior epigastric artery, which originates from the inferior mammary artery
- Lower rectus muscle is supplied by inferior epigastric artery, which originates from external iliac artery
- Blood supply
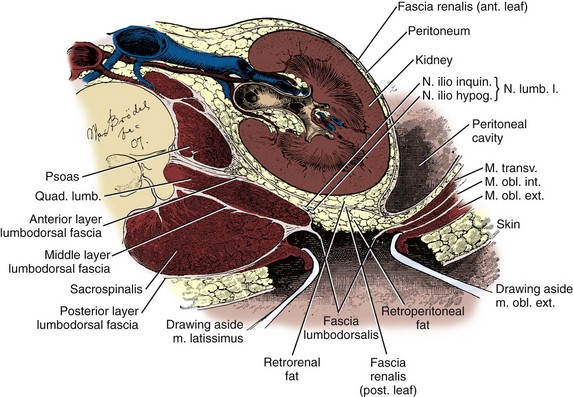
- Retroperitoneal space
- Lined posteriorly by the transversalis fascia, a thin layer posterior to the abdominal wall muscles and posterior to the posterior pararenal fat
Approaches to Open Kidney Surgery[edit | edit source]
Classification[edit | edit source]
- Flank (see Figure)
- 11th/12th rib supracostal
- 11th rib transcostal
- Thoracoabdominal
- Anterior 11th rib exposure
- Flank subcostal
- Foley muscle splitting
- Anterior (see Figure)
- Midline
- Subcostal (and extended subcostal)
- Bilateral subcostal (Chevron)
- Modified thoracoabdominal (hockey-stick)
- Transverse
- Paramedian
- Dorsal lumbotomy
{kind=link}
{kind=link}
Factors to consider[edit | edit source]
- Size of tumor
- Presence of thrombus
- Prior surgical history
- Patient body habitus
Flank approaches[edit | edit source]
- Advantages[3]
- Avoids entry into peritoneal cavity, minimizing bowel complications
- Direct access to kidney
- Disadvantages[4]
- Lateral incisions necessitate division of large muscle
- Risk of pleural injury
- Risk injuring intercostal nerves
- Risks of postoperative flank bulge, hernia, and significant pain
- Useful in[5]
- Partial nephrectomies
- Repair of ureteropelvic junction obstruction
- Open stone surgeries
- Drainage of renal or perirenal abscesses
- Avoid in
- Patients with pre-existing cardiopulmonary deficits
- Exaggerated lateral decubitus positioning may compromise pulmonary function and venous return to the heart.
- Patients with pre-existing cardiopulmonary deficits
- Position: ipsilateral lateral decubitus position
- After induction of anesthesia, insertion of an endotracheal tube, and introduction of a Foley catheter, the patient is moved on the table so that the ASIS is below the break of the table.
- In the classical flank position, the dependent 12th rib is directly over the kidney rest. Some surgeons do not use kidney rest.
- The patient is then positioned in ipsilateral lateral decubitus.
- The head is supported to avoid excess flexion at the cervical spine.
- The patient’s back is supported by a rolled blanket or surgical beanbag.
- To preserve stability and prevent forward roll, the dependent leg is flexed at the hip and knee and the top leg is kept straight. Two pillows should be placed between the legs, and both ankles should be padded.
- An axillary roll is deployed just caudal to the axilla and above the nipple line to prevent compression or injury of the brachial plexus.
- Any other pressure points are padded.
- The nondependent arm should be placed on a padded Mayo stand so that the arm is horizontal with slight forward rotation at the shoulder.
- The table is flexed between the iliac crest and costal margin until the flank muscles are under stretch.
- Optional: kidney rest is elevated in conjunction with table flexion.
- The bed is placed in Trendelenburg position so that the flank is rendered parallel to the floor.
- The patient is secured to the mobile part of the operating table with 2-inch-wide adhesive tape at the shoulder and the hip, which fixes the patient in place while allowing adjustment of flexion. Care should be taken to leave enough space for the self-retaining retractor.
- After induction of anesthesia, insertion of an endotracheal tube, and introduction of a Foley catheter, the patient is moved on the table so that the ASIS is below the break of the table.
11th/12th rib supracostal[edit | edit source]
- Can be used above the 11th or 12th ribs
- May be challenging to mobilize pleura without injury with approach above 11th rib
- Advantages
- Easier than flank 11th transcostal incision and may provide equal exposure
- Surgical description
- See video
- Incision
- Begin at the lateral border of the sacrospinalis muscle/posterior axillary line, at the superior aspect of the 12th or 11th rib
- The level of the incision is determined by the patient’s anatomy, the location of the lesion, and the planned procedure.
- Using cross-sectional imaging, a horizontal line drawn from the kidney over to the lateral edge of the rib marks the highest level that is easily accessed from that level of flank incision[6]
- The level of the incision is determined by the patient’s anatomy, the location of the lesion, and the planned procedure.
- Continuing anteriorly until the lateral border of the ipsilateral rectus abdominis muscle.
- If the incision is to be extended anteriorly, the patient may be rocked back 30 degrees with a rolled towel providing support behind the back.
- Begin at the lateral border of the sacrospinalis muscle/posterior axillary line, at the superior aspect of the 12th or 11th rib
- Enter retroperitoneum
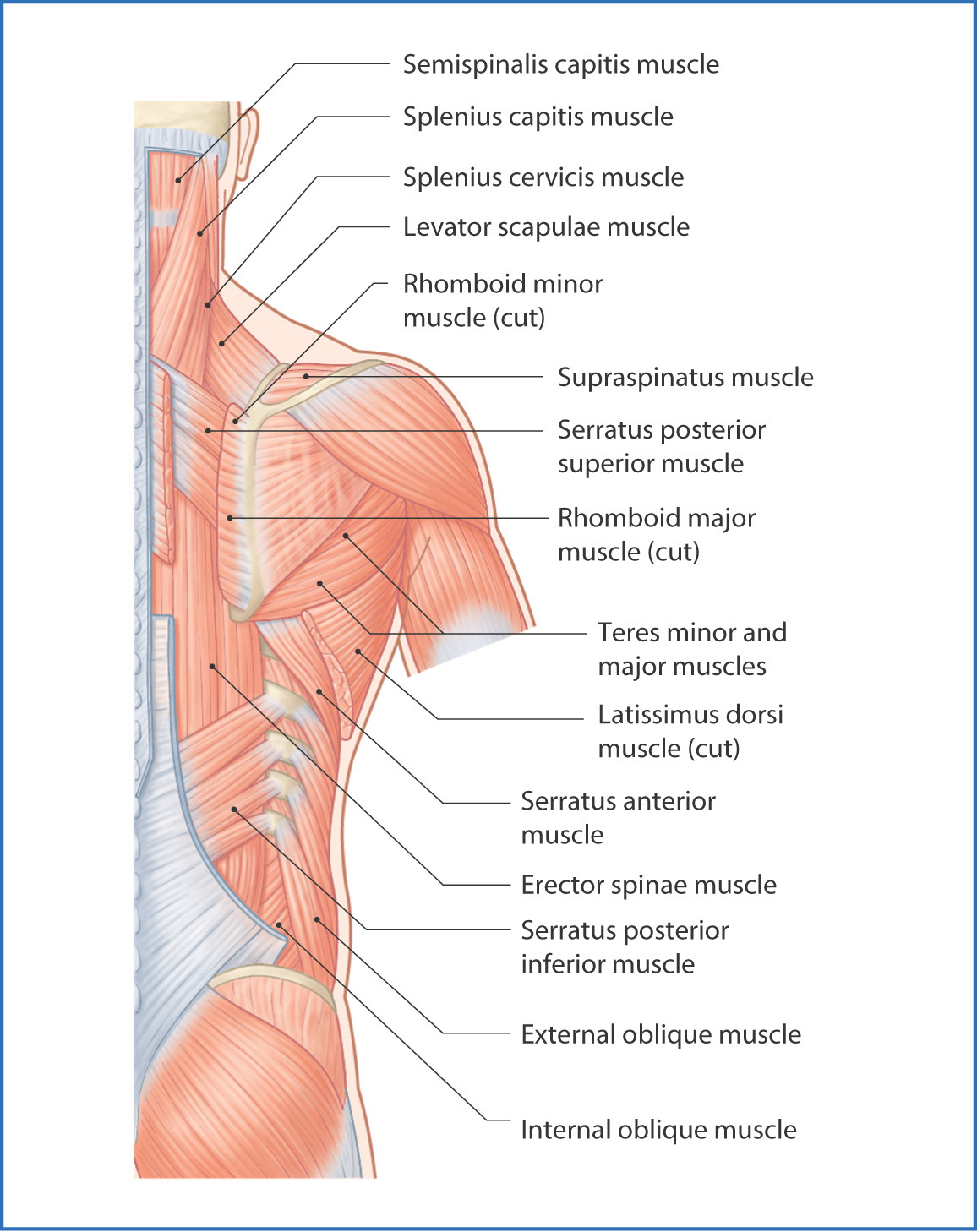
- Continue dissection through the subcutaneous tissue at the superior aspect of the rib to expose the latissimus dorsi posteriorly and external oblique muscles anteriorly (see Figure).
- In the posterior aspect of the incision, divide the latissimus dorsi to expose the posterior inferior serratus muscles (see Figure). Then, divide the posterior inferior serratus muscles to expose the intercostal muscles (see Figure).
- Anteriorly, divide the external oblique muscles to expose the internal oblique muscles. Then, divide the internal oblique muscles to expose the transversus abdominis muscle. As the 11th intercostal neurovascular bundle is encountered between the internal oblique and transversus abdominis, it is freed up and reflected superiorly. The transversus abdominis muscle fibers are separated in line with their fibers, while sweeping the peritoneum medially and inferiorly.
- The intercostal muscles above the 12th rib are carefully incised off the top edge of the rib beginning at its tip using cautery and proceeding posteriorly. The corresponding intercostal nerve is identified and spared. To avoid the neurovascular bundle, the intercostal muscles are divided in close proximity to the superior aspect of the rib.
- Lifting the tip of the rib, the attachments of the diaphragm are teased off of the underside of the upper edge of the rib with scissors, watching for the edge of the pleura, which is usually encountered a few centimeters back from the tip of the rib.
- The edge of the pleura is mobilized off the rib and is reflected superiorly while the intercostal nerve remains safe below the 11th rib
- Run the pad of the left index finger back along the top edge of the rib until it meets the sharp edge of the costovertebral ligament. Insert slightly opened heavy curved scissors, curve down, and hug the top of the rib with the blades to divide the ligament sharply, avoiding the intercostal bundle that lies below the upper (11th) rib.
- The lower rib can pivot down on its costovertebral joint and be retracted inferiorly to be held out of the way with a selfretaining retractor.
- Divide the lumbodorsal fascia at the tip of the rib to avoid both peritoneum and pleura (see Figure).
- Reflect the peritoneal envelope medially.
- Setup self-retaining retractor (e.g., Finochietto, Bookwalter, or Omni-Tract)
- Protect the ribs with moist sponges
- Develop pararenal space
- Bluntly develop the pararenal space
- Gently push the peritoneum anteromedially with a moist sponge stick to further develop the anterior pararenal space medially.
- Identify and ligate renal vessels
- Identify renal vein: for left-sided nephrectomy, open the anterior renal fascia overlying the aorta and dissect superiorly until the left renal vein is found. Using right angle dissection, place a vessel loop around the left renal vein for retraction. Palpate the vein for evidence of tumor thrombus. Dissect and mobilize the left renal vein while ligating its lumbar, adrenal, and gonadal branches with 3-0 silk. These branches of the left renal vein, particularly the lumbar branch, are common sources of operative hemorrhage during left nephrectomy.
- Identify renal artery: identify the left renal artery as it comes off the lateral surface of the aorta deep to the left renal vein, doubly ligate it with 2-0 silk, and then divide or take with a vascular staple load. With the left renal artery controlled, the left renal vein should decompress. If it remains engorged, the possibility of an accessory renal artery needs to be considered, and the lateral aorta should be further dissected before ligating the vein. Otherwise, the vein can be safely ligated with 2-0 silk and divided or taken with the vascular staple load.
- Completely mobilize the kidney outside of the renal fascia: start with the posterior pararenal space. Progress inferiorly and identify then divide the ureter while mobilizing the lower pole.
- Adrenalectomy/spare adrenal: pull the upper pole into the wound and dissect the adrenal gland off the superoanteromedial kidney, progressing laterally to medially. Alternatively, if adrenalectomy is indicated, identify and ligate the left middle adrenal artery on the lateral surface of the aorta. Proceed from the superolateral surface of the renal fascia medially, progressively clipping and dividing the attachments and blood supply to the left adrenal gland.
- Closure: Partially straighten the table, just enough to allow the edges of the wound to come together. If a drain is required, it is placed through a stab incision well below the 12th rib. A running or interrupted suture closure of the external and internal oblique fascial layers may be made with heavy absorbable or permanent suture in one or two layers, with care taken to avoid the intercostal neurovascular bundle below the rib
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Thoracoabdominal approach[edit | edit source]
- Useful in (4):
- Large renal masses
- Suprarenal or upper pole masses (for right-sided tumours, can push liver into chest)
- Renal tumors with venous extension
- Tumors involving adjacent structures.
- Surgical description
- Position: similar to flank approach (see above); the pelvis is rotated to a more horizontal position than for the flank incisions, at an angle of approximately 45 degrees.
- Skin incision
- Begins at the lateral aspect of the sacrospinalis muscle over the 10th or 11th rib
- Depending on the location of the tumor, access is gained through the 8th, 9th, 10th, or 11th intercostal spaces.
- Can continue and can travel as far as the contralateral rectus abdominis muscle or caudally toward the symphysis pubis.
- Begins at the lateral aspect of the sacrospinalis muscle over the 10th or 11th rib
- The internal oblique and transversus abdominis muscles are transected. The underlying peritoneum is opened, and the peritoneal cavity and chest are entered. Staying close to the superior border of the rib, the intercostal muscles are divided, which exposes the underlying pleura and diaphragm.
- The pleura is opened sharply, taking care to avoid the lung. The costovertebral ligament is divided. The diaphragm is opened from its thoracic surface. Starting anteriorly and proceeding posteriorly, the diaphragm is opened in a curvilinear fashion staying about two fingerbreadths from the chest wall to avoid injuring the more central phrenic nerve.
- The liver or spleen is gently retracted upward. Additional hepatic mobility can be obtained by dividing the coronary ligament and the right triangular ligament of the liver.
- For right-sided tumors, the kidney and great vessels are approached by mobilizing the colon medially and mobilizing the duodenum medially (kocherizing).
- For leftt-sided tumors, the kidney and great vessels are approached by mobilizing the colon and the tail of the pancreas.
Flank subcostal (sub 12th rib)[edit | edit source]
- Main disadvantage
- Poor access to the renal hilum
- Useful in
- Lower renal pole
- Ureteropelvic junction
- Proximal ureter
- Avoid in
- Large renal masses
- Partial nephrectomy
- Surgical description
- Skin incision
- Begins at the costovertebral angle, approximately at the lateral border of the sacrospinalis muscle just inferior to the 12th rib.
- Continuing onto the anterior abdominal wall a fingerbreadth below and parallel to the 12th rib.
- To avoid the subcostal nerve, the incision can be curved gently downward at the midaxillary line.
- INSERT FIGURE
- Continue dissection through the subcutaneous tissue to expose the fascia of the latissimus dorsi and external oblique muscles. Use electrocautery to incise the muscles in the line of the incision, starting with the latissimus dorsi posteriorly. The posterior inferior serratus muscles, which insert into the lower four ribs, are also encountered in the posterior portion of the wound and transected. In the anterior aspect of the wound the external oblique muscle is divided. These maneuvers expose the fused lumbodorsal fascia, which gives rise to the internal oblique and transversus abdominis muscles.
- Divide the lumbodorsal fascia and internal oblique muscle are divided (Fig. 60-6).
- The subcostal nerve should be identified between the internal oblique and transversus abdominis muscles and spared
- By using two fingers inserted into an opening created in the lumbodorsal fascia at the tip of the 12th rib, the peritoneum is swept medially as the transversus abdominis is split digitally.
- Skin incision
Anterior 11th Rib Exposure[7][edit | edit source]
- Extraperitoneal approach
- Advantages
- Smaller incision than flank incision
- Obviates need for rib removal
- Minimizes risk of pneumothorax
- Less pain than with a standard flank or transperitoneal incision
- Disadvantages
- Inability to examine intraperitoneal contents
- Slightly decreased exposure of hilum (compared to transperitoneal approach)
- Useful in
- Partial nephrectomy
- Small to moderate tumors that require radical nephrectomy and are not amenable to laparoscopic nephrectomy
- Position
- Semiflank torque position with the operative side and torso rotated medially 45° off the table, while the hips and lower extremities remain in a supine position
- The anterior superior iliac spine is placed just below the inferior aspect of the kidney rest. This allows for maximal exposure in the operative area after the table is maximally flexed and the kidney rest is elevated. The table is placed into a mild Trendelenburg position to keep the patient parallel to the floor. An axillary roll is placed as well as a posterior role to maintain the flank position. All extremities and pressure points are carefully padded and protected. The upper extremity, ipsilateral to the tumor, is placed onto a padded aeroplane arm board. The contralateral upper extremity is placed on a standard arm board. The patient is secured into position with the use of wide adhesive tape. The operative area is shaved and prepared with the agent of choice.
- Incision
- Plan incision along a straight line from the tip of rib 11 toward a mark 1 cm above the umbilicus
- Length of the incision is tailored individually for the patient’s body habitus and size of tumor
- Plan incision along a straight line from the tip of rib 11 toward a mark 1 cm above the umbilicus
- Step by step
- The ribs are palpated and identified. A marking pen is used to outline ribs 10, 11, and 12. A straight incision is made. Dissection is carried through the external oblique and internal oblique muscles laterally. The medial extent of the incision extends to the lateral aspect of the ipsilateral rectus muscle (Fig. 8a-1C and D). Should a larger incision be necessary, the rectus fascia can be opened and rectus muscle divided also
- The transversus abdominis muscle overlies the peritoneum and must be opened while the peritoneum is dissected off posteriorly to remain extraperitoneal. The cut edges of the internal oblique muscle are grasped with Alice clamps at the lateral edge of the incision and the transversus abdominis fascia is dissected off the posterior abdominal wall both inferiorly and superiorly. A handheld Richardson retractor allows for elevation of the anterior abdominal wall as a sponge stick or Kittner is utilized for mobilization of the peritoneum (Fig. 8a-1E and F). The transversus is incised taking care to not open the peritoneum. A self-retaining Buchwalter retractor is utilized to maintain exposure. Moistened laparotomy sponges are used to protect soft tissues from retractor damage. Blunt dissection is used to mobilize the peritoneum medially off of Gerota’s fascia. With adequate mobilization, the renal hilum becomes visible. Additional retractors are carefully placed to hold the peritoneum medially (Fig. 8a-1G). In right neprectomy, the second portion of the duodenum can be visualized and retracted medially. Closure is performed with Looped 0-PDS suture to reapproximate the internal oblique and rectus muscles. Inter�rupted 0 Vicryl sutures are used to reapproximate the external oblique fascia. Marcaine (0.5%) is infiltrated into the muscle, subcutaneous tissues, and along rib 11 medially for postop�erative analgesia. The skin can be closed with subcuticular closure or staples.
Anterior approaches[edit | edit source]
- Advantages[8]
- Familiar to most surgeons
- Open and closure are very rapid
- Able to evaluate other intraabdominal organs
- Rapid access to the renal hilum
- Good control of the aorta/IVC if they are injured
- Reduced pain by avoiding muscle division
Anterior midline[edit | edit source]
- Advantages (in addition to above)
- Less painful than flank or transverse abdominal incisions that require division of major muscle groups
- Disadvantages[9]
- Limited exposure to the kidneys because of the renal hilum is at the upper limit of the incision
- Overlying colon, liver, and spleen must be mobilized widely
- Risk of late bowel obstruction and incisional hernia
- Indications
- Renal trauma
- Permits exploration for associated intraperitoneal injuries.
- Bilateral renal procedures
- Both ureters must be accessed (e.g. retroperitoneal fibrosis)
- Renovascular surgery
- Reconstructive procedures, including ileal ureteral replacement
- Horseshoe kidney
- Renal trauma
- Step-by-step[10]
- Position: supine, with the table extended at the patient's waist
- Incision: midline, from the xiphoid to just below the umbilicus
- Enter peritoneal cavity: divide the subcutaneous tissue down to the level of the fascia and identify the linea alba. Incise the linea alba to expose the preperitoneal fat covering the peritoneum. Grasp of the preperitoneal fat, ensuring that bowel is not taken with it, and sharply cut through the peritoneum layer. The remainder of the posterior rectus fascia and peritoneum may be opened, taking care to avoid any potential adhesions between the bowel and the anterior abdominal wall.
- Identify renal vessels: expose the posterior peritoneum by displacing the patient’s small bowel contents to the right and the descending colon to the left.
- Make an incision in the posterior peritoneum over the aorta, between the fourth portion of the duodenum and the inferior mesenteric vein (IMV).
- This area is devoid of vessels arising off of the anterior aorta as long as one stays above the takeoff of the inferior mesenteric artery (IMA).
- Continue dividing superiorly over the aorta up to the left renal vein.
- The renal vein is dissected above and below with care taken not to injure the superior mesenteric artery (SMA); the SMA should be on the anterior surface of the aorta and is usually 1 to 2 cm cephalad to the left renal vein.
- The left and right renal arteries are usually encountered coursing directly lateral off the aorta posterior to the left renal vein though multiple arteries may arise anywhere from above the level of the SMA down to the common iliac arteries
- Make an incision in the posterior peritoneum over the aorta, between the fourth portion of the duodenum and the inferior mesenteric vein (IMV).
- Approach to kidneys:
- Incise along the lateral edge of the colon on the avascular line of Toldt, continuing up around the hepatic flexure (right) or splenocolic ligament (left).
- On the right side, the second portion of the duodenum is encountered after medialization of the colon. The duodenum is then medialized (Kocher maneuver) over the aorta, which exposed the anterior aspect of the IVC
- On the left side, the upper limit of Gerota fascia must be separated from the lower edge of the pancreatic tail and splenic hilum.
- After abdominal contents are mobilized off Gerota fascia, a self-retaining retractor can be placed to keep the intestines out of the way for the remainder of the surgery.
- Incise along the lateral edge of the colon on the avascular line of Toldt, continuing up around the hepatic flexure (right) or splenocolic ligament (left).
- Closure
- One-layer closure
Anterior Subcostal[edit | edit source]
- Advantages[11]
- Excellent access to the upper pole and adrenal gland
- Good exposure to renal hilum
- Lower risk of pleurotomy and pneumothorax compared to standard flank incision
- Disadvantages[12]
- Limited visibility, best reserved for small renal tumors or benign conditions
- Better anterior access may be gained from extending incision to other approaches such as the hockey-stick, extended subcostal or bilateral subcostal (Chevron)
- Prolonged ileus or delayed small bowel obstruction secondary to adhesion formation from manipulation of the bowel[13]
- Limited visibility, best reserved for small renal tumors or benign conditions
- Step-by-step[14]
- See video
- Left side is extraperitoneal approach while right side is transperitoneal approach??
- Spleen and peritoneal contents can be readily mobilized anteriorly on left side??
- Liver limits ability to mobilize peritoneum off Gerota fascia on right side??
- Position
- Supine with table slightly flexed at the patient's waist (anterior superior iliac spine at the level of the kidney rest)
- A small roll can be placed behind the patient on the operative side, rotating the patient slightly.[15]
- If preferred, the shoulder can be turned 30-40 degrees and the ipsilateral arm placed over the head on support
- Supine with table slightly flexed at the patient's waist (anterior superior iliac spine at the level of the kidney rest)
- Incision
- Medial extent: midline anteriorly (through the ipsilateral rectus), one third of the distance from the xiphoid to the umbilicus
- Lateral extent: at the tip of the 11th rib near the anterior axillary line
- If the exposure is inadequate, further exposure can be gained by extending the incision
- Medially and incising the opposite rectus sheath slightly (extended subcostal)
- Converting it to a hockey-stick
- Converting it to a full bilateral subcostal (Chevron)
- Posteriorly as a flank incision
- If the exposure is inadequate, further exposure can be gained by extending the incision
- Two fingerbreadths from the costal margin[16]
- Use cautery/scalpel to incise along length of incision
- After incision of the Scarpa fascia, use cautery to dissect through external oblique muscle (and overlying fascia) and anterior rectus sheath.
- Excellent hemostasis is essential to prevent delayed bleeding and hematoma formation.
- Use cautery to dissect through internal oblique muscle (and overlying fascia) and rectus muscles.
- Rectus muscle may be divided with electrocautery, making sure to control the superior epigastric artery
- Digitally separate the fibers of the transversus abdominis, starting as far laterally as possible, where the peritoneum is less adherent
- Left side: extraperitoneal approach
- Enter extra-peritoneal space
- Divide the left side of the anterior rectus sheath and the external oblique muscles for a short distance
- Divide the internal oblique muscles
- Digitally separate the fibers of the transversus abdominis, starting as far laterally as possible, where the peritoneum is less adherent
- Incise the transversalis fascia
- Develop extra-peritoneal space
- Displace peritoneum. Free the peritoneum off above and below the incision. Sweep the peritoneum bluntly off the abdominal wall laterally and inferiorly to the iliac crest. Continue posteriorly to the lateral edge of the psoas muscle in the extraperitoneal space and bluntly strip the peritoneum from the underlying muscle layer. Sharp dissection with scissors may be required.
- To develop the plane between the peritoneum and the anterior leaf of Gerota fascia, incise the transversalis fascia just outside the reflection of the peritoneum laterally. This should be a filmly, fibroareolar tissue in an avascular plane, and the gonadal and ureter should remain posteriorly
- Identify, divide and ligate renal vessels
- Renal vessels may be encountered at the level of the aorta
- Mobilize kidney
- Gerota fascia is divided above the kidney, carefully mobilizing it off of the lower edge of the pancreas
- Lower limit of Gerota is divided above the common iliac artery, and the ureter and gonadal vessels are divided
- The remaining posterior and medial attachments are divided, and the kidney is removed with Gerota fascia
- Deliver specimen
- Closure: two-layers
- First-layer: internal oblique
- Second-layer: external oblique and rectus fascia
- Enter extra-peritoneal space
- Right side: transperitoneal approach
- Enter peritoneal space
- Use Debakey forceps to lift up on peritoneum and enter peritoneum with Metzenbaum scissors. Place finger inside and extend incision over finger.
- Divide the peritoneum in an area free of underlying bowel or the the midline and extend to expose the liver, ascending colon, and greater omentum covering the transverse colon
- The ligamentum teres is doubly ligated and incised to allow for maximal exposure.
- The peritoneum is visually and manually examined to evaluate for metastatic disease. The retroperitoneum and perinephric space are entered by mobilizing the colon with incision of the white line of Toldt while retracting the colon medially. The assistant utilizes a handheld Richardson retractor to lift the anterior abdominal wall improving access to the White line.
- After mobilization of the colon, a self-retaining Buchwalter retractor is placed
- Use Debakey forceps to lift up on peritoneum and enter peritoneum with Metzenbaum scissors. Place finger inside and extend incision over finger.
- Identify, divide and ligate renal vessels
- Renal vessels may be approached through the posterior peritoneum as described for above midline transperitoneal
- Alternatively, incise along the lateral border of the hepatic flexure and mobilize the right colon and duodenum medially to expose the kidney
- Renal vessels may be approached through the posterior peritoneum as described for above midline transperitoneal
- Mobilize kidney
- Medialize the colon: Incise the posterior parietal peritoneum on the line of Toldt from the common iliac artery to the hepatic flexure. Develop the anterior pararenal space by dissecting in the plane anterior renal fascia and the mesentery of the ascending colon
- This step may be difficult if large or inflammatory masses as the anterior pararenal space may be obliterated by tumor or occupied by numerous large collateral vessels
- Important to stay out of the ascending mesocolon because injury to the right colic or ileocolic arteries (and their branches) can devitalize this segment of the colon
- Mobilize the hepatic flexure of the colon using sharp and blunt dissection to minimize the risk of hepatic capsular tear and to improve visualization of the upper pole and adrenal gland. The hepatorenal ligament is also incised to allow the upper pole of the kidney to fall away from the liver. The Falciform ligament is also incised to allow the liver to be retracted without injury.
- Medialize the duodenum (Kocher maneuver): The second part of the duodenum may be closely connected to the medial part of the tumor, and is useful for mobilizing it farther medially and away from the mass.
- The duodenum is fragile and is in danger of injury, with necrosis and perforation as a consequence. Avoid using electrocautery around the duodenum, but, if necessary, light bipolar coagulation can safely achieve hemostasis
- Identify IVC: Incise the anterior renal fascia on the medial aspect of the kidney and identify the IVC
- Identify renal vein: dissect anteriorly on the IVC, both cranially and caudally, until the left renal vein, right renal veins, and right gonadal vein are identified. Dissect the right renal vein and place a vessel loop around it so that it can be gently and atraumatically retracted
- Palpate the renal vein and IVC for evidence of tumor thrombus
- Identify and ligate renal artery: The right renal artery is usually located deep and superior to the right renal vein on the lateral side of the IVC. If possible, dissect around the right renal artery using a right angle clamp. Stay close to the vessel and spread the perivascular tissue using the right angle clamp or Metzenbaum scissors. Use 2-0 silk ties or a vascular staple load to ligate the renal artery.
- If the right renal artery is hard to isolate because tumor is encroaching medially on the renal hilum or because troublesome hilar bleeding is occurring, identify the artery in the interaortocaval region and control it with either a 2-0 silk or vascular staple load. This provides much better exposure to the right renal artery lateral to the IVC, which can then be ligated and divided.
- In the interaortocaval region, watch for lumbar veins that come into the renal vein or vena cava at this level. When you encounter them, do not secure them with clips that may become displaced or preclude the ability to use a stapler, but pass a 0 silk suture on a right angle clamp and tie it.
- Bluntly develop the posterior pararenal space. Normally, this is easily done by gently sliding the left hand underneath the kidney while retaining contact with the fascia of the muscles of the posterior abdominal wall. Small vessels in the posterior pararenal space that perforate through the posterior renal fascia should be clipped or cauterized as this plane is gently developed.
- Occasionally, the renal tumor will invade the psoas muscle posteriorly, making the posterior dissection difficulty. In these circumstances, ensure that the renal pedicle is adequately controlled before dissected the tumor away from the muscle sharply.
- Bluntly dissect the inferior pole of the kidney (with its investing fat and renal fascia).
- Identify and ligate the ureter. Doubly ligate it with 2-0 silk or large clip and then divide it, or take it with an additional staple load.
- Identify the gonadal vein and protect it by gently pushing it medially.
- This vein is friable, and its avulsion from the IVC is a common cause of hemorrhage during nephrectomy
- Dissect the inferomedial kidney away from the IVC until it is free up to the renal hilum superiorly.
- With the exception of the upper pole, the entire kidney with the perirenal fat and renal fascia intact should now be mobilized
- Dissect the upper pole of the kidney. Grasp the kidney with the left hand and gently pull it caudally into the wound to expose the upper pole attachments, working laterally to medially, free the kidney from its cranial attachments.
- Consider adrenalectomy vs. adrenal-sparing.
- If adrenalectomy is indicated, remove the gland en bloc with the kidney, within the renal fascia.
- If the adrenal can be spared, dissect it off the anterior, superior, and medial surface of the kidney
- The cranial connections to the adrenal gland must be divided carefully step by step between clips or by using a join vessel sealing and dividing device or stapler. Clip the small vessels and especially the lymphatics.
- If the adrenal gland is injured, oversew the edge with 4-0 monocryl on a tapered half-circle SH needle.
- Beware of the short right adrenal vein that typically enters the IVC posterolaterally, high in the retroperitoneum, near the hepatic veins. If avulsed, this small vein can lead to significant hemorrhage before it is controlled.
- Deliver specimen
- Closure
- looped 0-PDS to reapproximate the rectus and internal oblique muscles. The external oblique fascia is reapproximated using interrupted 0-Vicryl sutures. The incision is infiltrated with 0.5% Marcaine and the skin is closed with subcuticular closure or staples.
- Medialize the colon: Incise the posterior parietal peritoneum on the line of Toldt from the common iliac artery to the hepatic flexure. Develop the anterior pararenal space by dissecting in the plane anterior renal fascia and the mesentery of the ascending colon
- Enter peritoneal space
Bilateral subcostal (Chevron)[edit | edit source]
- Composed of bilateral anterior subcostal incisions
Advantages[edit | edit source]
- Provides access to both sides of the retroperitoneum
Disadvantages[edit | edit source]
- Limited exposure to lower abdomen and pelvis
Useful in[edit | edit source]
- Renovascular surgery
- Radical nephrectomy with inferior vena cava (IVC) tumor thrombectomy or tumor extension into liver, spleen, or pancreas.
- Outstanding exposure of the renal pedicles and great vessels.
- For kidney tumors with extensive thrombus requiring access to the chest, a cephalad median sternotomy extension can be made (Mercedes incision) providing full access to the heart
- Bilateral renal tumors
- Bilateral nephrectomies for large polycystic kidneys
Technique[edit | edit source]
- Position: supine with abdomen hyperextended over a break
- See Figure: Incision L
- See Video
- Skin incision
- Begins at the tip of the 11th rib
- Continues approximately two fingerbreadths below and parallel to the costal margin, curves superiorly in the midline, travels parallel to the contralateral costal margin, and terminates at the tip of the contralateral 11th rib.
- Divide anterior abdominal wall muscles
- Divide both sides of the anterior rectus sheath
- Insert a finger under the rectus muscle and divide it with cautery, taking care to control the epigastric artery
- The superior epigastric artery runs along the deep surface of the rectus abdominis[17]
- Divide the external and internal oblique muscles and split the fibers of the transversus abdominis muscle
- Enter peritoneum
- Incise the transversalis fascia and peritoneum
- Complete the incision against one or two fingers inside the abdomen
- Divide the falciform of the liver between two clamps, ligating each end or using a vessel-sealing device
- Exposure of the kidneys and retroperitoneum on the right and left sides is identical to that described earlier (midline transperitoneal incision)
- Closure
- Straighten the table
- Place a holding sure in to approximate the linea alba in the midline, which is tied after fascia closure is completed
- The incision may be closed in a single layer, including the anterior and posterior rectus sheaths, or multiple layers incorporating the peritoneum and posterior rectus fascia in one layer and the internal and external oblique fascial layers laterally with addition of the anterior rectus sheath medially
{kind=link}
Modified thoracoabdominal (hockey-stick)[edit | edit source]
- Extraperitoneal approach
- Transverse portion of the incision facilitates development of the extraperitoneal space
- Position
- Begin with patient supine with table flexed at the waist
- Place the patient in the modified flank position with the ipsilateral arm suspended over the chest and a roll beneath to elevate the ipsilateral side slightly
- Incision
- May be extended inferiorly all the way to the pubic bone or laterally over the rib case as a thoracoabdominal incision
- Divide the subcutaneous tissues and anterior rectus fascia in line with the incision
- Divide the body of the rectus muscle at the upper edge of the incision
- Divide the external oblique, internal oblique, and transversalis muscle near the costal margin
- Enter retroperitoneum, lateral to the peritoneal reflection
- The peritoneum can be swept off the anterior abdominal muscles medially before the posterior rectus fascia is opened
- The abdominal wall flap can then be retracted inferiorly with a towel clamp
- The peritoneal envelope is them mobilized laterally back to the psoas while superiorly the peritoneum is mobilized off the diaphragm
- The plane between the peritoneum and the anterior leaf of Gerota fascia is most easily identified near the lower pole and is developed by incising the thin fascial layer that envelops them together
- The remainder of the avascular plane is developed bluntly using fingers or a Kittner, reflecting the entire peritoneal envelope medially
- The kidney, ureters, and gonadal vessels with Gerota fascia remain atop the psoas muscle
- A self-retraining retractor such as a Bookwalter allows the peritoneum to be kept medially out of the way
- Closure
- The transverse portion of the incision is closed in two layers, with care taken to keep the corner properly aligned
11th rib transcostal[edit | edit source]
- Involves removal of the 11th rib
- Used in
- Simple or partial nephrectomy
- Simple adrenalectomy
- Steo-by-step
- See video
Dorsal lumbotomy[edit | edit source]
- Useful in
- Pediatric patients
- Thin adults requiring bilateral nephrectomy
- Main advantage: low morbidity since no muscle is transected.
- Anatomic approach to the kidney, with incision of fascial planes rather than muscle.
- Main disadvantage: lack of exposure, particularly to the renal hilum and its vessels
- Surgical description
- Position: prone
- Incision: vertical skin incision from the inferior border of the 12th rib to the iliac crest, in line with the lateral border of the sacrospinalis muscle.
- [Further details in Campbell’s]
Surgery for benign diseases[edit | edit source]
- Simple nephrectomy
- Definition: removal of the kidney without Gerota fascia
- Used to manage nonmalignant diseases of the kidney
- Indications
- Intractable symptoms or associated problems, such as bleeding, pain, hypertension, or persistent infection.
- Durable non-function or poor function of a kidney as a result of obstruction, infection, trauma, stones, nephrosclerosis, vesicoureteral reflux, polycystic kidney, or congenital dysplasia.
- Open nephrostomy
- Extracorporeal renal surgery with auto-transplantation
- Rarely used in contemporary urologic practice, since open in situ renal exposure with vascular clamping and hypothermia provides excellent access to the kidney for nearly all forms of renal surgery.
- Currently, reserved for reconstruction of complex renal pathologies in cases of a solitary kidney, when percutaneous approaches are not appropriate or possible, and when routine in situ operative exposure is inadequate
Surgery for malignancy[edit | edit source]
Radical nephrectomy[edit | edit source]
- Definition: removal of kidney outside of Gerota fascia
- Important to stay outside Gerota’s (perifascial) to prevent postoperative local tumor recurrence because ≈25% of clinical T1b/T2 RCCs demonstrate perinephric fat involvement
Indications[edit | edit source]
- Tumors in non-functional kidneys
- Large tumors replacing the majority of renal parenchyma
- Tumors associated with detectable regional lymphadenopathy
- Tumors associated with renal vein thrombus
Radical nephrectomy with adrenalectomy
- See Management of Localized and Locally Advanced Kidney Cancer Chapter Notes
Radical nephrectomy with lymphadenectomy
- See Management of Localized and Locally Advanced Kidney Cancer Chapter Notes
- Regional lymphadenectomy
- Includes ipsilateral great vessel and interaortocaval regions, extending from the crus of the diaphragm to the common iliac artery
- For right-sided renal masses when lymphadenectomy is considered, the paracaval, precaval, retrocaval, and interaortocaval nodes from the right crus of the diaphragm to the bifurcation of the IVC are sampled.
- Employed in select cases of advanced local disease and when technically feasible
- Includes ipsilateral great vessel and interaortocaval regions, extending from the crus of the diaphragm to the common iliac artery
- Surgical description (for right-sided lymphadenectomy)
- Right-side lymphadenectomy
- A right-angle clamp and electrocautery are used to split the lymphatic tissue from the anterior surface of the IVC. The lymphatic tissue is cleared cranially from the right crus of the diaphragm (located 3 to 4 cm above the right renal vein) and caudally until the bifurcation of the IVC.
- The right gonadal vein is ligated at its insertion into the IVC with 2-0 silk suture, in order to avoid avulsion of the vein. Next the lymphatic tissue is cleared off the lateral aspect of the IVC (paracaval nodes).
- The IVC is gently elevated with a vein retractor to expose the lumbar branches. The lumbar veins (typically four or five branches on either side of the IVC) are carefully ligated with 3-0 silk ties and transected.
- The lymphatic trunks located above the renal vein are ligated with surgical clips.
- Care to adequately ligate the lymphatic trunks is essential since large quantities of lymph and chyle drain through the cisterna chyli and thoracic duct, and failure to appropriately control them can result in chylous ascites .
- Once the lumbar veins are secured and the superior aspect of the lymphatic trunk above the renal vein is secured, the assistant rolls the IVC medially with gentle pressure using two sponge sticks. Next the lymphatic tissue is cleared off the retrocaval region. The nodal tissue overlying the anterior surface of the aorta is then split and divided to the superior border of the left renal vein. Division of the nodal packet is followed to the medial border of the IVC and the aortocaval nodal packet is cleared to the level of the common iliac vessels.
- Left-side lymphadenectomy
- For left-sided renal masses, the lymphatic tissue on the anteromedial surface of the aorta is clipped and divided and rolled laterally. The split is continued cranially along the aorta to the level of the superior mesenteric artery (SMA) and caudally past the inferior mesenteric artery (IMA) to the bifurcation of the aorta.
- While the SMA and the celiac trunk have to be preserved, the IMA can be tied and divided in case of involved lymphadenopathy.
- Once the lymphatics are dissected off the anterior and lateral surface of the aorta, the assistant gently elevates the aorta on either side to expose, secure, and divide the lumbar arteries. Once the lumbar arteries are properly secured, the aorta is rolled medially and the tissue between the anterior longitudinal vertebral ligament and the aorta (retroaortic lymph nodes) is resected.
- The interaortocaval nodes are resected only if they are palpable or visualized on preoperative imaging, or if there is extensive nodal involvement around the aorta.
- For left-sided renal masses, the lymphatic tissue on the anteromedial surface of the aorta is clipped and divided and rolled laterally. The split is continued cranially along the aorta to the level of the superior mesenteric artery (SMA) and caudally past the inferior mesenteric artery (IMA) to the bifurcation of the aorta.
- Right-side lymphadenectomy
Surgical description[edit | edit source]
- Important to keep the renal fascia intact to ensure complete resection and to avoid tumor spillage
- The most commonly used incision for radical nephrectomy is the subcostal flank incision
- Incise through the skin and muscular layers. Setup Bookwalter retractor. If right-sided, the liver and gallbladder are packed away superiorly. When additional mobilization of the liver is required, the avascular right triangular ligament is incised.
- Incise the posterior parietal peritoneum on the white line of Toldt from the pelvis (region of the iliac artery) to the upper quadrant (region of hepatic/splenic flexure).
- Develop the anterior pararenal space by dissecting in the plane between the anterior renal fascia and the mesentery of the ascending/descending colon.
- Important to avoid injury to the ascending mesocolon, since injury to the right colic and ileocolic arteries may devitalize this segment of colon.
- Important to resect the renal fascia in its entirety for the best chance of surgical cure and to avoid any intra-abdominal tumor spillage.
- Mobilize the hepatic/splenic flexure of the colon using sharp and blunt dissection
- Mobilize the duodenum/tail of pancreas medially with extreme care.
- With medially located tumors, mobilization of the duodenum should be performed with extreme care.
- Identify the IVC/aorta posteriorly.
- Identify the renal vein. Dissect along the anterior surface of the IVC/aorta to identfy the renal vein (and gonadal vein if right-sided)
- On the right side, gonadal vein drains into IVC just below renal vein. On left side, gonadal vein drains into left renal vein.
- Placement of a vessel loop will enable gentle traction of the renal vein.
- The renal vein is palpated for any tumor thrombus.
- Surgical clips do not provide adequate hemostasis for the lumbar veins.
- Identify the renal artery, posterior to the renal vein.
- The origin of both renal arteries are generally found posterior to the left renal vein after it is mobilized after the aorta
- The origin of the right renal artery is posterior to the left renal vein and IVC.
- The left renal artery is usually located cranial and posterior to the left renal vein.
- If identification of the renal artery is difficult, attention is turned to the lower pole of the kidney to identify the ureter and gonadal vein.
- The left gonadal vein can be traced to its insertion to help identify the left renal vein.
- Depending on the size and location of the tumor, determine whether the left gonadal vein should be left intact or tied off and transected to help with mobilization of the kidney. If technically feasible, the gonadal vein is spared. However, often because of the large size of the renal tumor, the gonadal vein cannot be safely left intact without the risk of avulsion from the IVC (right side) or left renal vein.
- With ligation of the ureter, the kidney is lifted from a posterior to an anterior position in order to aid in identification of the renal artery posterior to the kidney.
- Another option for identifying the right renal artery in difficult hilar dissections is to dissect in the interaortocaval region at its takeoff from the aorta
- For left radical nephrectomy, particularly for upper pole renal masses, identification of the left renal artery from the posterior approach is recommended to avoid inadvertent ligation of the superior mesenteric artery, which is on the anterior surface of the aorta 1 to 2 cm cephalad to the left renal vein.
- The origin of both renal arteries are generally found posterior to the left renal vein after it is mobilized after the aorta
- Divide hilar vessels. Once the renal artery and vein are identified, the renal artery is ligated with two right-angle clamps and divided. Preferably, the proximal end of the renal artery is clamped with two right-angle clamps and the distal end with one right-angle clamp. The renal artery is divided using a fine scalpel. The proximal end is ligated with 0 silk suture and further secured with 2-0 silk suture ligature; the distal end is tied with 0 silk tie. With the renal artery secured and divided, the renal vein is secured and divided in a similar fashion.
- The most common source of bleeding after division of the renal hilum on the left is a lumbar vein.
- Hem-o-locks are contraindicated for arteries
- Whole-pedicle clamp
- May be utilized to control the hilar vessels at times when the renal artery and vein may not be able to be separated individually because of significant hilar lymphadenopathy.
- En bloc ligation of the whole renal pedicle may be associated with with a risk of arteriovenous fistula
- Some small clinical series have not found any evidence of such fistulas in patients undergoing nephrectomy who have been managed by en bloc stapling of the renal hilum.
- Emergent condition of loss of control of the renal hilar vascular pedicle
- Important to stay calm. Inform the anesthesiologist and all operating room personnel of major bleeding and request aggressive hydration and availability of blood products.
- Compression can be applied using a fingertip or sponge stick to achieve hemostasis as best as possible so that the rest of the operating room staff can prepare. Compression can also be applied on the IVC and/or aorta to control bleeding.
- Two Yankauer suction tubes can be used to clear the surgical wound.
- Vascular occlusion clamps are used to clamp and ligate actively bleeding vessels. Clamping should not be done blindly; rather, one should suction, pack, retract, and dissect to get better exposure.
- If the bleeding is occurring from the renal artery, compress the aorta above the renal artery, clamp the arterial stump with a vascular clamp, and repair the defect with two layered running vascular sutures.
- If the bleeding is occurring from the IVC because of an avulsed or lacerated renal vein, or avulsed gonadal or lumbar vein, place a finger on the hole until the hole can be grasped with an Allis clamp. Pulling up on the clamp will normally stop the bleeding, allowing the defect to be visualized for repair.
- Wound closure
- Investigate for hemostasis and evaluate adjacent organs for any signs of injury.
- The diaphragm and pleura are tissues that can be inadvertently injured secondary to retraction during radical open renal surgery.
- To test for pleural injury, the retroperitoneum is filled to the level of the flank incision with saline. The anesthesiologist then inflates the lungs with high inspiratory volumes. Bubbling of saline irrigation in the retroperitoneum with deep inspiration would suggest a pneumothorax.
- In case of a small pleural injury, the pleural cavity can be closed with running nonabsorbable sutures. Prior to complete closure of the pleura, the tip of a 14-Fr red rubber catheter is placed in the pleural cavity. The end of the catheter is placed in a saline-filled bowl. The anesthesiologist provides a deep inspiratory breath to evacuate any air from the pleural cavity through the red rubber catheter and into the saline bowl. Once the air is evacuated from the pleural cavity as evidenced by bubbles in the saline bowl, the red rubber catheter is removed and the assistant cinches the pleural incision tight for an airtight closure. A postoperative chest radiograph is essential to assess for any significant pneumothorax, even in cases when pneumothorax is not suspected.
- Fascial closure
- For subcostal incision, the fascial layers are approximated typically in two layers—the transversus abdominis and internal oblique fasciae are approximated together, and the external oblique fascia is approximated as a separate layer.
- The subcutaneous tissue is approximated using 3-0 absorbable sutures. The skin is approximated with skin staples or subcuticular 4-0 poliglecaprone 25 (Monocryl) suture
- Investigate for hemostasis and evaluate adjacent organs for any signs of injury.
Complications[edit | edit source]
- Injury to the GI vasculature
- The celiac trunk supplies the esophagus, stomach, pancreas, liver, spleen, and part of the duodenum
- The superior mesenteric artery supplies the small bowel, cecum, ascending and transverse colon
- The inferior mesenteric artery supplies the transverse, descending, and sigmoid colon
- The inferior mesenteric artery can be safely ligated as long as the marginal artery of the colon is patent and can supply blood from the SMA to the left colonic arcades
- Ligation of either the SMA or the celiac trunk is a catastrophic event that occurs predominantly with left-sided nephrectomy and that must be rapidly reversed if the patient is to survive.
- The inferior mesenteric vein (IMV) is found in the mesentery of the descending colon, immediately lateral to the ligament of Treitz. The IMV can be safely ligated during surgery without consequence. In contrast, the superior mesenteric vein (SMV) should not be ligated unless that is the only surgical option. The abdomen should not be closed primarily in cases of SMV injury because abdominal compartment syndrome will occur.
- Injury to the liver and spleen:
- Small splenic or hepatic injuries (capsular tears and minor lacerations) can usually be managed effectively by electrocautery or argon beam coagulation. Fibrin glue and topical hemostatic meshes (e.g., Surgicel) are useful adjuncts.
- More serious splenic injuries can be managed by splenorrhaphy or splenectomy
- Minor hepatic lacerations can be repaired using the same basic principles as for a partial nephrectomy closure.
- Injury to bowel
- Minor electrocautery or laceration injuries should be managed by careful debridement of the nonviable tissue and closure in two layers, the mucosal layer with continuous 4-0 chromic or Vicryl suture on a 1 2 circle tapered needle, and the serosa and muscularis layer with 3-0 silk interrupted suture on a 1 2 circle tapered needle. An omental flap is placed over the injury and a closed suction drain is inserted
- Injury to the pancreas:
- First step is a thorough inspection of the pancreas
- Superficial lacerations and contusions can usually be managed by applying fibrin glue and inserting a closed suction drain. The drain is monitored for an alkaline pH and lipase/amylase levels to determine whether a pancreatic fistula is developing.
- If the injury to the pancreas is deep and/or involves the pancreatic duct, consultation with a gastrointestinal surgeon is essential for appropriate repair and management.
- Pulmonary complications:
- Large postoperative pleural effusions can be managed by aspiration initially, followed by chest tube drainage if necessary
- Chylous ascites
- Results from disruption of the major para-aortic lymphatic channels leading to the cisterna chyli and is predominantely noted in left-sided procedures (radical or donor nephrectomy) or RPLND
- Patients classically have abdominal distention without significant pain or fevers and will have normal bowel habits.
- Diagnosed by paracentesis with ascitic fluid found to have classically white and turbid appearance with fluid analysis showing elevated lymphocytes, associated with a high cholesterol and triglyceride content.
- Initial treatment is to reduce the flow of chyle into the lymphatics by a low-fat medium-chain triglyceride diet
- If chylous ascites persists despite dietary management, the next step should involve bowel rest and TPN with the concurrent use of octreotide, a somatostatin analog.
- Somatostatin has been documented to significantly decrease postprandial increase in TG levels by inhibiting lymphatic flow
- Open or laparoscopic treatment using suture ligation and fibrin glue to control the leak can be pursued if conservative management fails.
- Intraoperatie location of the lymphatic leakage can be challenging and the combined use of preoperative lymphangiography and consumption of “fatty” meal immediately before surgery has been documented to be beneficial in helping the surgeon locate the site of the leak
Partial nephrectomy[edit | edit source]
Contraindications[edit | edit source]
- Patient-related issues
- Uncontrolled coagulopathy
- Cancer-related issues
- Diffuse encasement of renal pedicle by tumor
- Diffuse invasion of central collecting system
- Tumor thrombus involving major renal veins
- Adjacent organ invasion (stage cT4)
- Regional lymphadenopathy (stage cTxN1)
- Technical issues
- Cold ischemia time > 45 minutes (consider extracorporeal approach)
- Less than 20% of global nephron mass retained
Preoperative considerations[edit | edit source]
- Hyperfiltration injury: when a significant portion of renal parenchyma is removed, the renal blood flow is delivered to a smaller number of nephrons, which can lead to increased glomerular capillary perfusion pressure that results in an increased single-nephron glomerular filtration rate called hyperfiltration. Over decades, the hyperfiltration can injure the remaining nephrons, resulting in focal segmental glomerulosclerosis and the clinical manifestations of proteinuria and progressive renal failure.
- Renal ischemia and hypothermia: To minimize blood loss and allow for adequate surgical visibility, it is often necessary to employ vascular compression during partial nephrectomy. Manual and clamp compression of renal parenchyma is preferable, since vascular clamping is associated with a higher incidence of renal complications. It is unclear whether leaving the renal vein unclamped for retrograde renal perfusion offers any tangible benefit. Attempting to limit warm ischemia to 20 minutes and cold ischemia to 35 minutes helps maintain renal function
- Adequate renal hypothermia (core renal temperature of 20° C) takes at least 15 minutes to achieve if the kidney is packed with ice slush. To help prevent acute postoperative renal failure, intravenous mannitol (12.5 g) and furosemide (20 mg) should be infused about 15 minutes before renal artery clamping. While evidence supporting this practice is somewhat limited, both drugs are quite well tolerated in a well-hydrated patient§§
- Intravenous mannitol helps prevent tissue damage by preventing cellular edema.
Summary of steps[edit | edit source]
Enucleation (for small tumours)[edit | edit source]
- Two cylinder shaped cigarette-like bolsters are prepared by rolling Nu-Knit Absorbable Hemostat (Ethicon, Cincinnati, OH) and tying each end with absorbable sutures. Two pledgets are prepared by folding Nu-Knit into a double-layer strip 5 to 10 cm wide and 1 cm long.
- The kidney is exposed using either the anterior subcostal or flank approach as described earlier. The entire surface of the kidney is freed of perirenal fat, with the exception of the perirenal fat overlying the tumor. While removing the perirenal fat, special care should be taken to avoid injury to the ureter, particularly for lower pole tumors.
- Intravenous mannitol and furosemide are administered and the renal pedicle is exposed sufficiently to allow safe application of a vascular clamp if necessary. Vessel loops are placed around the renal vein and artery individually.
- The renal cortex surrounding the tumor is marked circumferentially using electrocautery. The plane outside the tumor pseudocapsule and within the normal parenchyma is identified and bluntly dissected with small closed Metzenbaum scissors. For enucleation of small lesions, renal occlusion is usually not necessary. However, if there is excessive bleeding that hampers proper visualization of the resection margin, then manual compression of the kidney or clamping of the renal pedicle can help. When small vessels within the kidney are encountered they are divided sharply with scissors. The tumor is excised and the margins are examined for gross evidence of a positive surgical margin
- Small bleeding vessels in the renal parenchyma are controlled with 4-0 absorbable figure of-eight sutures on a tapered needle or by coagulation with an argon beam coagulator or bipolar electrocautery. The integrity of the collecting system is verified by checking for injury and repairing with absorbable suture if necessary.
- A Nu-Knit pledget that was prepared earlier is placed along each border of the excised renal parenchyma and in the bottom of the excised parenchyma (Fig. 60-40). The defect is closed with 2-0 absorbable horizontal mattress sutures on a long tapered 1 2 circle needle.
- If clamping was used, the pedicle is unclamped and inspection is done for bleeding, ischemia, or urine leakage of the kidney and for adjacent organ trauma. The perirenal fat and renal fascia are replaced around the kidney. A closed suction drain in the pararenal space is placed to monitor for bleeding and urine leaks. The closed suction drain is removed after 2 to 5 days when the output is minimal. A Foley catheter is used to monitor the urine output. Unless there is a large renal collecting system defect, a ureteral stent is not typically required.
Wedge resection (for large cortical tumours)[edit | edit source]
- For large tumors, intravenous mannitol and furosemide are administered, then the renal artery is clamped with a vascular bulldog clamp. Based on the surgeon’s preference, when partial nephrectomy is being performed for larger tumor sizes or lesions that are close to the renal hilum, the renal vein may also be clamped after clamping the renal artery to provide better hemostasis during partial nephrectomy. A plastic bag or sheet is placed around the kidney and filled with ice slush. The kidney is allowed to cool to 20° C (approximately 15 minutes).
- The renal capsule is circumferentially incised 5 to 10 mm peripheral to the tumor with electrocautery. Using a combination of blunt and sharp dissection with Metzenbaum scissors, the tumor is excised with a small rim of normal parenchyma. The specimen is inspected for visible tumor at the resection margin, then submitted for frozen-section analysis.
- Bleeding vessels are controlled with figure-of-eight sutures or with argon beam or bipolar electrocautery. The deep resection margin of the kidney must be inspected for any residual tumor or any sign of collecting system injury. If there is any doubt about collecting system injury, 10 to 20 mL of diluted indigo carmine is injected into the renal pelvis while occluding the ureter to assess for leaks. The collecting system is closed with 4-0 absorbable suture on a tapered needle.
- The renal parenchymal defect is reconstructed using Nu-Knit bolsters and pledgets as described above. Fibrin glue is applied to the renal parenchymal defect. Finally, the renal vessels are unclamped—if the renal vein as well as the renal artery is clamped, the renal vein is unclamped first followed by unclamping the renal artery.
- [Further details in Campbell’s]
Segmental nephrectomy (for large polar tumours)[edit | edit source]
- Intravenous mannitol and furosemide are administered and the renal pedicle is completely dissected, including the segmental branches.
- A bulldog clamp is applied to the apical segmental artery (or basilar segmental artery for lower pole tumors) and the line of ischemia is observed. The avascular line can be further demarcated by injecting 5 mL of indigo carmine directly into the clamped artery. The line of ischemia is the optimal site for transection of the kidney and should be lightly marked with electrocautery. The apical segmental artery is ligated, then the renal pedicle is clamped en bloc with a curved Satinsky clamp. A plastic bag or sheet is placed around the kidney and filled with ice slush to cool the kidney to 20° C (approximately 15 minutes). The renal capsule is incised along the line of ischemia with electrocautery. Using blunt dissection, the pole of the kidney is excised. Bleeding vessels are controlled, working expeditiously and accurately. The clamp is released to check for uncontrolled bleeders. If hemostasis is adequate, collecting system repair is begun; otherwise the pedicle is reclamped and vascular control resumed.
- The collecting system is inspected for injury. If the defect in the collecting system is large, a guidewire is inserted into the defect and manually guided into the ureter and bladder. A 6-Fr double-J ureteral stent is inserted over the guidewire with the proximal coil in the renal pelvis. The collecting system is closed with a running 4-0 absorbable noncutting suture.
- The renal capsule is closed using Nu-Knit pledgets and horizontal mattress sutures as described earlier. Because the defect is large, we use a larger needle (e.g., XLH, GS-27) for segmental polar nephrectomies and heminephrectomies than for enucleation and wedge resections. Nephropexy should be considered if the kidney is quite mobile; however, injury to retroperitoneal nerves overlying the psoas and quadratus lumborum muscles must be avoided. The kidney is covered with perirenal fat and renal fascia and a closed suction drain is placed to monitor output postoperatively. The indwelling Foley catheter is removed when the patient is mobile and stable. Depending on the output of the closed suction drain, it can be removed 5 to 10 days postoperatively. If a ureteral stent is used, it should not be removed for 4 to 6 weeks postoperatively. After removal of the indwelling Foley catheter, if the output of the closed suction drain is increased, the transurethral indwelling Foley catheter is reinserted to reduce the intrapelvic urine pressure, which should minimize the output from the closed suction drain.
Post-operative care[edit | edit source]
- A retrospective cohort study of 154 patients undergoing partial nephrectomy for kidney cancer found that patients that received ketorolac had an earlier return to solid diet and earlier discontinuation of patient controlled analgesia, and no difference in serum creatinine, blood loss, transfusion rates and complication rates, compared to patients that did not receive ketorolac[18].
Complications[edit | edit source]
- Urinary fistulae
- PNs that involve of the collecting system increase the possibility of urinary leakage.
- Most urinary fistulae present themselves in ≈1 week postoperatively; in cases of deep renal resections, it is advisable to keep the closed suction abdominal drain in place for 7-10 days.
- In the case of an unrecognized or delayed urinary leak, the presence of an adjacent urinoma will prevent fistula closure and predispose the patient to infection/abscess formation.
- Percutaneous drainage of the urinoma is the preferred method used to control an unrecognized or delayed pyelocutaneous fistula.
- To further maximize drainage, consider a double-J ureteral stent that is placed after retrograde pyelography and (3) a Foley catheter to keep the entire collecting system at low pressure.
- Most fistulas resolve within 4 to 6 weeks with conservative management, and reoperation is rarely required.
- Percutaneous drainage of the urinoma is the preferred method used to control an unrecognized or delayed pyelocutaneous fistula.
- Postoperative bleeding
- Delayed bleeding can occur following partial nephrectomy
- Usually, bleeding segmental and subsegmental arteries can be selectively embolized and the kidney salvaged without need for complete nephrectomy.
- Life-threatening hemorrhage can also occur and require complete angioinfarction of the kidney or reoperative exploration.
- Renal insufficiency
- While most cases of postoperative renal insufficiency are mild and temporary, some cases require hemodialysis for electrolyte and fluid management. Hyperfiltration injury can also cause a gradual decrease in renal function over time, typically associated with proteinuria.
- The medullary thick ascending limb of Henle is most sensitive to ischemic damage.
IVC Thrombectomy[edit | edit source]
- Usually, IVC thrombectomy is accompanied by radical nephrectomy and regional lymph node dissection
- Classification of IVC thrombi
| Thrombus level | Incidence rate in RCC | Proportion of thrombi | Cranial extent of thrombus | Management of tumour thrombus |
| 0 | 12% | 65% | Confined to renal vein | Radical nephrectomy |
| I | 2% | 10% | Within 2 cm of renal vein ostium | IVC milking, partial IVC occlusion,
ostial cavotomy |
| II | 3% | 15% | Below hepatic veins | Complete IVC mobilization/control,
infrahepatic cavotomy |
| III | 1% | 5% | Between hepatic veins and diaphragm | Complete occlusion: suprahepatic
IVC clamping, infrahepatic cavotomy Partial occlusion: veno-venous bypass, infrahepatic cavotomy |
| IV | 1% | 5% | Above diaphragm | Deep hypothermic arrest, infrahepatic cavotomy, right atriotomy |
- See graphic representation of thrombus level
Pre-operative considerations[edit | edit source]
- Anticoagulation
- Patients with kidney cancer are at increased risk of pulmonary embolism as a result of malignancy-associated hypercoagulability and venous thrombus embolization.
- Intravenous or low-molecular-weight heparin should be started as soon as tumor thrombus is detected
- Potential benefits (3):
- Reduce risk of pulmonary embolism
- Tumour thrombus shrinkage
- Bland thrombus shrinkage and/or prevention
- Evidence supporting the use of preoperative anticoagulation is limited
- Temporary suprarenal IVC filters are also an option for patients with level 0, I, and II tumor thrombi. However, suprarenal IVC filters are not recommended because of the risk of contralateral renal and hepatic vein thrombosis, the risk of provoking embolization, and the impediment that these devices can pose to future IVC thrombectomy.
- Potential benefits (3):
- Preoperative angioembolization
- Can be considered to attempt to shrink the thrombus and facilitate surgery
- Indications (4):
- Caval thrombi appears to invade the IVC
- Thrombus is associated with a bleeding kidney
- When deep hypothermic arrest is planned since the patency of the coronary arteries can be simultaneously assessed with angiography
- Thrombus invades the intrahepatic or suprahepatic veins and cannot be excised
- Angiographic infarction of the blood supply to the tumor thrombus can help shrink a large thrombus to a more manageable size, potentially avoiding the need for bypass or extensive mobilization of the liver.
- In ≈1/3 of cases, tumour thrombi have an independent blood supply arising from the renal artery and/or aorta.
- Timing
- Optimal timing for angioembolization is unknown but at most centers, when undertaken, it is usually performed 1 day prior to surgery.
- Complications
- Iatrogenic pulmonary embolization of the tumor thrombus when angiography is performed; however, this risk appears to be minimal.
- Ischemia-related flank pain
- Tumor lysis syndrome
- Multidisciplinary Approach
- Urologists who do not routinely handle the IVC and aorta should consult a vascular surgeon for level II and III thrombi to aid in vena caval control and reconstruction.
- Consultation with a cardiothoracic surgeon preoperatively for all level III and IV thrombi is essential, since access to the mediastinal compartment for vascular bypass and thrombus removal may be required.
- Involvement of a cardiologist or cardiac anesthesiologist is essential for level II to IV thrombi to allow for intraoperative TEE.
- Intraoperative use of transesophageal echocardiography (TEE) for level II to IV thrombi is recommended given the risk of intraoperative thrombus detachment and the possibility of interval thrombus growth in the period immediately preceding surgery.
- Surgical approach
- Tailored to the level of IVC thrombus. In general:
- Level I thrombi are isolated by a Satinsky clamp and are thus readily addressed
- Level II thrombi require sequential clamping of the caudal IVC, contralateral renal vasculature, and cephalad IVC along with mobilization of the relevant segment of the IVC and occlusion of lumbar veins. The renal ostium is then opened and the thrombus is removed, all in a bloodless field.
- Level III thrombi may require mobilization of the liver and exposure of the intrahepatic IVC to allow the thrombus to be mobilized caudad to the hepatic veins, and venous isolation can then proceed as for a level II thrombus.
- Level IV thrombi have traditionally been managed with cardiopulmonary bypass and hypothermic circulatory arrest
- A hypocoagulable state follows when coming off the pump following hypothermic circulatory arrest. This is associated with increased risks of cerebrovascular accident and myocardial infarction
- Hypothermic circulatory arrest is still the preferred approach in complex cases but some centers are now trying to avoid it
- When tumor thrombus invades the wall of the vena cava, aggressive resection of the involved cava and attainment of negative surgical margins are required to minimize the risk of recurrence. IVC grafting or reconstitution is required in some instances.
- Tailored to the level of IVC thrombus. In general:
Level 1 vena caval thrombectomy[edit | edit source]
- Can usually be treated in a similar fashion to level 0 thrombi by reducing the thrombus into the renal vein
- Usually, level I thrombi are partially occlusive, are nonadherent, and do not require extensive IVC dissection or any form of bypass.
- Surgical plan
- Position: anterior midline or anterior subcostal
- Step-by-step
- Position a self-retaining retractor
- Medialize the colon and develop the anterior pararenal space
- Identify and expose the great vessels and the renal hilum
- Identify and ligate the renal artery
- Renal artery can be ligated in the intera-ortocaval region, if right-sided, or para-aortic if left-sided
- Take care care not to manipulate the renal vein or IVC too much.
- Secure the renal artery with 0 silk ligature or a large clip.
- Ligating the renal artery early will help reduce the blood flow to the kidney and minimize the amount of potential blood loss.
- Gently mobilize the kidney outside the renal fascia, divide the ureter, and dissect the IVC above the right renal vein.
- Some groups mobilize the kidney after the thrombectomy is complete, in order to minimize the risk of embolization, while others mobilize the kidney first followed by thrombectomy
- Identify and secure the contralateral renal vein, suprarenal IVC, and infrarenal IVC with vessel loops.
- To help with temporary ligation of these vessels, 3- to 6-inch portions of an 18-Fr red rubber catheter are passed through the vessel loop and used as Rummel tourniquets.
- While this degree of vascular control may not be necessary for all level I thrombi, it is prudent to have adequate vascular control if there is any doubt about the extension of the level of thrombus.
- Starting cranially, the IVC is gently pinched closed, and then the Rummel tourniquets are applied so that the infrarenal IVC, contralateral renal vein, and suprarenal IVC are closed in that order.
- To help with temporary ligation of these vessels, 3- to 6-inch portions of an 18-Fr red rubber catheter are passed through the vessel loop and used as Rummel tourniquets.
- Using the left hand, milk the IVC toward the ostium of the renal vein. Place a C-shaped Satinsky vascular clamp around the ostium of the renal vein partially occluding the IVC, ensuring that the thrombus is located within the jaws of the clamp before complete closure.
- Palpate the IVC for evidence of any other thrombus.
- Suction and two sponge sticks (to compress the IVC if necessary) are readied and laparotomy sponges are placed around the renal vein to collect any spillage of tumor thrombus after opening of the renal vein.
- Incise the renal ostium circumferentially using a scalpel or fine-tipped Metzenbaum or Potts scissors.
- Extract the thrombus by gentle downward traction on the renal vein.
- A gauze is wrapped around the renal vein stump and secured with a silk ligature to prevent tumor spillage.
- Dissect medial and other remaining attachments of the kidney
- Deliver specimen
- Inspect the IVC for evidence of residual thrombus
- Close the IVC defect with a running closure using a 4-0 Prolene suture on a BB vascular needle.
- Prior to tying the knot, ask anesthesia to apply positive airway pressure, then pinch the infrarenal IVC closed and release the Satinsky clamp. Allow 5 to 10 mL of blood to escape from the caval defect to flush out any residual thrombus fragments and debris before pulling the suture tight and tying the closure.
- A regional lymphadenectomy is performed, irrigating the wound copiously with sterile water.
- Consider placement of a closed suction catheter to monitor for bleeding.
Level II vena caval thrombectomy[edit | edit source]
- Surgical plan (for left-sided tumor)
- Position: anterior midline and chevron incisions provide the best access for left-sided tumors associated with tumor thrombi in the IVC.
- Exposure for a tumor thrombus associated with a left-sided tumor is more difficult since the IVC is best accessed from the right retroperitoneum.
- Both the right and the left colon have to be mobilized to get adequate exposure.
- Exposure for a tumor thrombus associated with a left-sided tumor is more difficult since the IVC is best accessed from the right retroperitoneum.
- Medialize the left colon and develop anterior pararenal space.
- Identify and ligate the left renal artery near its origin close to the aorta.
- Identify and ligate the adrenal, lumbar, and gonadal branches of the left renal vein. These branches are often dilated and friable and occasionally contain thrombi.
- Mobilize the kidney outside the renal fascia and divide the ureter.
- Medialize the right colon, small bowel, and duodenum
- Develop the right anterior space
- Expose the great vessels.
- Carefully dissect the IVC to its bifurcation, ligating the right gonadal vein on its anterior surface.
- To gain 2 to 3 cm of extra infrahepatic IVC exposure, accessory hepatic veins are ligated to the caudate lobe (this is an optional maneuver).
- Obtain vascular control sequentially in the following order:
- Ligate the ipsilateral (left) renal artery
- Clamp the infrarenal IVC
- Clamp the contralateral (right) renal vein
- Clamp the suprarenal IVC
- Optionally, one can clamp the contralateral renal artery to prevent renal engorgement while the venous outflow is temporarily clamped.
- More of an issue for left-sided tumors since unlike the left kidney, the right kidney does not have significant venous collateralization to shunt blood when the right renal vein is clamped.
- While obtaining vascular control, one must be very gentle to avoid dislodging the thrombus.
- Ligate and divide the lumbar veins, as required.
- Prior to clamping, some may use 0.5 mg/kg of intravenous heparin to prevent clamp-related thrombotic complications. This may increase bleeding and some do not routinely heparinize our patients.
- Optionally, one can clamp the contralateral renal artery to prevent renal engorgement while the venous outflow is temporarily clamped.
- Excise the renal vein ostium circumferentially excised and extend the incision superiorly onto the anterior surface of the IVC using Potts scissors.
- Use a Penfield dissector to carefully extract the tumor thrombus from the IVC.
- Lumbar veins can be a source of troublesome bleeding at this stage and should be ligated or sutured as needed
- Remove the gross tumor thrombus and kidney en bloc.
- Irrigate IVC lumen with heparinized saline (100 units/mL) and inspect the intima for signs of caval invasion. Any suspicious areas should be biopsied or resected.
- Close the caval defect with a running 4-0 Prolene suture.
- The IVC lumen can be safely narrowed to about 50% of its preoperative size without requiring special measures.
- Prior to tying the knot, the infrarenal clamp is released and 5 to 10 mL of blood is allowed to seep from the cavotomy to clear the IVC of air and debris.
- After tying the suture, the contralateral renal vein clamp is released followed by the suprarenal IVC clamp.
- Position: anterior midline and chevron incisions provide the best access for left-sided tumors associated with tumor thrombi in the IVC.
- When performing right radical nephrectomy with tumor thrombectomy, the suprarenal IVC can be resected, but only if the left renal vein has been ligated distal to its venous tributaries (i.e., gonadal, lumbar, and adrenal veins). This will allow the left renal vein to drain through these tributaries. Given the lack of venous tributaries on the right side, the suprarenal IVC should not be resected for a left-sided tumor unless one provides alternative venous drainage for the right kidney with autotransplantation or a saphenous vein graft to the splenic, portal, or inferior mesenteric vein.
- Regional lymphadenectomy is performed, consideration is given to leaving a closed suction drain, and the wound is irrigated and the incision closed.
Level III-IV vena caval thrombectomy: intra-abdominal approach[edit | edit source]
- Pre-operative planning
- Operating room should be set up for possible cardiopulmonary bypass (CPB), including deep hypothermic arrest.
- Intraoperative TEE
- Should be available to measure the cranial extent of the thrombus and to monitor the thrombus for fracture and embolization.
- Cardiac function is evaluated with TEE so that the anesthesiologist can appropriately manage the patient’s hemodynamics.
- The key decision for level III thrombi is whether to attempt an intra-abdominal thrombus extraction with complete hepatic mobilization or use a combined intrathoracic/intra-abdominal approach with bypass.
- This decision can only be made intraoperatively, after the renal artery is ligated, the liver is mobilized, and the IVC is exposed and evaluated.
- It is preferable to clamp the IVC below the hepatic veins, since the venous return from the liver is significant.
- As a rule of thumb, patents with free-floating partially occlusive thrombi will not tolerate suprahepatic clamping very well and should probably undergo bypass. Contrarily, patients with completely occlusive thrombi will typically have developed extensive collateral venous drainage networks and therefore tolerate clamping much better.
- Occasionally, a level IV thrombus can be milked into the abdomen through a small diaphragmatic incision and treated intra-abdominally.
- It is crucial that IVC control not compromise the operation since bleeding and hypotension can lead to an incomplete tumor resection, a result that is universally fatal.
- Surgical plan
- Position: anterior midline incision for level III and IV thrombi; a chevron incision with added sternotomy can also be used.
- Expose the right kidney and great vessels, as described for a level I thrombus
- Ligate the right renal artery is ligated in the interaortocaval area.
- Dissect the infrahepatic IVC is gently.
- Isolate the infrarenal IVC and left renal vein and Rummel tourniquets are placed around them.
- Mobilize the liver
- Ligate and divide the ligamentum teres, the remnant of the obliterated left umbilical vein that is located at the lower free border of the falciform ligament.
- Divide the falciform ligament up to the upper border of the liver where it branches into the coronary ligament on the right and the left triangular ligament on the left.
- Divide the superior layer of the coronary ligament with scissors or electrocautery, taking care not to injure the liver or the IVC, which is located just behind the ligament in the bare area of the liver. Division of the superior layer of the coronary ligament continues along the right border of the liver until it forms the right triangular ligament (the fused superior and inferior layers of the coronary ligament), which should also be divided. Mobilization of the right lobe of the liver is completed by dividing the inferior layer of the coronary ligament, the attachment that ties the liver to the diaphragm, upward toward the IVC.
- The left triangular ligament is divided anteriorly and hepatic mobilization is completed by dividing the posterior aspects of the left triangular ligament toward the IVC. The right lobe of the liver can now be safely and gently rotated toward the midline so that the IVC can be evaluated on the posterior surface of the liver. For tumors of the left kidney, it may be necessary to divide the diaphragmatic attachments of the spleen so that it can be rotated toward the midline with the pancreas without being traumatized.
- Develop the plane between the posterior surface of the liver and the anterior surface of the IVC.
- The help of a hepatic surgeon with this portion of the procedure should be considered.
- This plane contains venous branches from the liver that are divided into upper and lower groups.
- The most important group is the upper group that contains the right, middle, and left hepatic veins, the principal outflow from the liver, and therefore cannot be divided. Tumor thrombus can extend into these veins and they must be carefully inspected and cleared of any thrombus during thrombectomy. Obstruction of these three veins leads to the Budd-Chiari syndrome.
- The lower group of hepatic veins (the accessory hepatic veins) drain blood principally from the caudate lobe (with a small contribution from the right lobe) and can be safely divided. The accessory hepatic veins are ligated with 2-0 silk and the plane between the IVC and the liver is developed.
- Additionally, the lumbar veins are ligated with 2-0 silk and the plane between the IVC and the posterior abdominal wall is developed. The IVC should now be fully mobilized.
- Create a window in the lesser omentum and encircle the porta hepatis (also called the portal triad or hepatic pedicle), which contains the portal vein, common hepatic artery, and common bile duct, with a Rummel tourniquet.
- Clamping the porta hepatis (the Pringle maneuver) is necessary to prevent massive blood loss if the IVC is clamped above the major hepatic veins.
- Clamping the IVC above and below the hepatic veins while performing a Pringle maneuver is called total hepatic vascular occlusion.
- If the IVC is clamped below the major hepatic veins and the accessory hepatic veins are ligated, the Pringle maneuver may not be necessary.
- Under normothermic conditions, the porta hepatis can be clamped for up to 60 minutes, although a clamping time of 20 minutes or less is preferred since ischemic hepatic injury and portal vein thrombosis can ensue. Another complication of the Pringle maneuver is splenic engorgement and rupture as a result of backup of venous drainage from the splenic vein, which normally empties into the portal vein.
- Determine the resectability of the tumor and thrombus is using TEE and a thorough intraoperative assessment of the anatomy.
- If the thrombus is below the hepatic veins or can be milked below these veins, it is usually safe to proceed without bypass.
- If the thrombus involves the hepatic veins or extends above the liver, bypass is often required.
- The IVC is occluded above the liver and thrombus and the patient’s hemodynamic response is observed over 2 to 5 minutes.
- Clamping the suprahepatic IVC results in a 60% reduction in cardiac preload, an increase in peripheral vascular resistance of 80%, an increase in heart rate of 50%, a drop in cardiac output of 40%, and a drop in mean arterial blood pressure of 10% to 20%. If the cardiac output drops more than 50% or the mean arterial blood pressure drops more than 30%, the patient will not tolerate suprahepatic IVC clamping. Options for managing this situation include bypass (our preference) and clamping of the supraceliac aorta.
- If the IVC clamping trial is tolerated and the thrombus can be removed in less than 30 minutes, it is safe to proceed with the intra-abdominal procedure.
- In sequence, the infrarenal IVC, the contralateral (left) renal vein, the porta hepatis, and the suprahepatic IVC are clamped.
- For left-sided tumors, the right renal artery should be clamped prior to the right renal vein since there is no good collateral venous drainage for the right kidney.
- Incise the ostium of the right renal vein is circumferentially and extend the incision toward the intrahepatic IVC.
- The incision should be large enough to permit extraction of all of the tumor thrombus and careful inspection of the intima of the IVC.
- Excise the thrombus and kidney.
- With the help of a Penfield dissector the IVC is cleared of adherent thrombus.
- If involved with tumor that cannot be scraped away, the IVC should be completely or partially resected and reconstructed (see below).
- A Fogarty balloon catheter (Edwards Lifesciences Corporation, Irvine, CA) or 20-Fr Foley catheter can be used as an embolectomy catheter if the thrombus is out of reach.
- With the help of a Penfield dissector the IVC is cleared of adherent thrombus.
- Close the IVC is closed as described for level II thrombus. The hepatic ligaments are tacked back into place to prevent torsion of the liver.
- A regional lymphadenectomy is performed and a closed suction drain is inserted.
Level III-IV vena caval thrombectomy: combined intra-abdominal and intrathoracic approach[edit | edit source]
- Level III thrombi that cannot be removed intra-abdominally and most level IV thrombi are managed with a combined intraabdominal and intrathoracic approach.
- Pre-operative planning
- A cardiothoracic surgeon needs to participate with the planned operation.
- Surgical plan:
- Thoracoabdominal, chevron laparotomy with sternotomy, and anterior midline laparotomy with sternotomy incisions can be used to provide access to the chest and abdomen
- Abdominal portion of the case is identical to the intraabdominal approach described above.
- Once the abdominal phase is completed, the cardiothoracic surgeon is called to the operating room and a median sternotomy is performed. The pericardium is opened and the right heart exposed. Often, mobilization of the liver and IVC is easier once the sternotomy is completed.
- Obtain bypass using one of the techniques described below.
- Once on bypass, the ostium of the renal vein is circumferentially excised, the incision is extended cranially on the IVC, and the thrombus is extracted.
- A right atriotomy is usually performed to help remove the suprahepatic thrombus.
- The atrium and IVC are then closed.
- The patient is taken off bypass and thoracotomy tubes and closed suction abdominal drains are placed.
- The hepatic ligaments are tacked back into place to prevent torsion of the liver and regional lymphadenectomy is performed.
- Bypass techniques for IVC surgery
- Bypass should be considered in patients in whom the IVC cross-clamping trial causes significant hypotension, as well as in patients in whom there is preoperative cardiac or hepatic dysfunction, contralateral renal dysfunction, or portal venous hypertension, and when there is major intraoperative bleeding that is difficult to control.
- Venovenous bypass
- Involves shunting the venous blood from below the renal veins to the venous return of the heart with the aid of a pump
- Advantage
- Least invasive bypass technique for IVC thrombi; can be done without opening the chest, unlike traditional cardiopulmonary bypass.
- 2 main options are available for infrarenal cannulation:
- Percutaneous approach through the femoral vein
- Direct intraoperative approach through the IVC just above its bifurcation.
- When cannulating the IVC, it is important to position the tip of the cannula as far from the tumor thrombus as possible to avoid dislodging it, which can cause a massive pulmonary embolism, and to avoid aspirating and recirculating tumor cells.
- Several options are available for delivering the shunted blood back to the heart: a percutaneous approach via the internal jugular vein, a cutdown approach to the brachial/axillary vein, and a direct intraoperative approach through the right atrium.
- Cardiopulmonary bypass +/- deep hypothermic arrest
- Cardiopulmonary bypass can be performed with or without deep hypothermic arrest.
- Cardiopulmonary bypass with deep hypothermic arrest involves stopping the heart and starting bypass, cooling the patient to 16° C to 18° C, and draining all of the blood from the patient.
- Advantages
- Can be used in cases in which the thrombus cannot be milked below an intrapericardial IVC clamp
- No need to clamp the aorta or porta hepatis or to ligate as many lumbar and hepatic veins since blood flow to these structures is no longer present. However, all vessels that have been traumatized or transected must be controlled since they will bleed once the patient is taken off bypass.
- Absence of active blood flow allows for complete inspection of the IVC and hepatic veins, thereby aiding in achieving a complete thrombectomy.
- Risk of embolization during thrombectomy is lower.
- Purpose of deep hypothermic arrest is to reduce organ metabolism, allowing for greater duration of absence of blood flow
- At normothermia, brain injury occurs after approximately 4 minutes of circulatory arrest. Most patients tolerate 30 minutes of deep hypothermic circulatory arrest without significant neurological dysfunction. Above 60 minutes, the majority of patients will suffer irreversible brain injury.[19]
- Disadvantage
- Very invasive
- Surgical plan:
- Mobilize the kidney and dissect IVC.
- The cardiothoracic surgeon performs the sternotomy, opens the pericardium, and exposes the heart and its vessels.
- Heparin-bonded cannulae are placed in the infrarenal IVC and the right atrium to collect venous blood and a cannula is placed into the aortic arch for outflow.
- The patient is heparinized and bypass is started.
- The aorta is clamped and cardioplegia solution is administered.
- The temperature of the recirculated blood is dropped to 10° C to 14° C and the patient is cooled for 15 to 30 minutes until a core temperature of 16° C to 18° C is reached.
- Intraoperative electroencephalography should be performed to determine when the brain has been adequately cooled.
- When sufficient cooling has been achieved, the perfusion pump is stopped and 95% of the patient’s blood volume is drained into the pump reservoir.
- Tumor thrombectomy should be performed as fast as possible, taking great care to ligate all potential bleeders.
- If the resection is taking longer than anticipated, the surgeon should consider allowing a 10-mL/kg/min trickle of blood to flow to the organs or using retrograde cerebral perfusion.
- If the patient has known coronary artery disease, coronary artery bypass can be performed at the same time.
- Once the IVC and right atrium are repaired, warm blood is reinfused from the pump reservoir and cardiopulmonary bypass is restarted.
- Hemostasis is performed while the patient warms to 37° C over the next 30 to 45 minutes.
- Once the heart has restarted pumping, bypass is stopped, the cannulae are removed, and protamine sulfate is administered.
- Most common difficulty associated with hypothermia and circulatory arrest is hemorrhage associated with platelet and clotting factor dysfunction
- Fresh frozen plasma, platelets, and packed red blood cells should be available to administer.
- Thoracostomy tubes and closed suction abdominal drains are inserted.
- Advantages
- Cardiopulmonary bypass with deep hypothermic arrest involves stopping the heart and starting bypass, cooling the patient to 16° C to 18° C, and draining all of the blood from the patient.
- Alternatives to CPB may include venovenous bypass and extensive liver mobilization
- Cardiopulmonary bypass can be performed with or without deep hypothermic arrest.
- Patching, replacing, and interrupting the IVC
- Patch Cavoplasty
- If the IVC lumen is expected to be < 50% of its original size, a patch cavoplasty is necessary to prevent IVC stenosis and thrombosis-related events
- Autologous and bovine pericardium, polytetrafluoroethylene (PTFE), collagen-impregnated Dacron (DuPont, Wilmington, DE), and autologous saphenous vein are materials that can be used for patch cavoplasty.
- Vena caval replacement
- In situations when a circumferential section of IVC has been removed or if a vena cava defect is too large for simple patching, vena caval replacement is necessary
- Typically, PTFE grafts are used to replace the IVC, although others have described spiraled saphenous vein, superficial femoral vein, and tubularized pericardium as options
- Postoperatively, low-dose intravenous heparin or a reduced dosage of low-molecular-weight heparin is given. Once the patient’s bowel function has recovered, lifelong oral warfarin is used with a target INR of 2 to 3.
- Patch Cavoplasty
- IVC filtration and permanent interruption for bland thrombus
- Occasionally, a patient with an infrarenal bland thrombus requires management at the time of tumor thrombectomy.
- For bland thrombus that is limited to the pelvic veins, intraoperative placement of an infrarenal vena cava filter is indicated.
- For bland thrombus that diffusely involves the infrarenal IVC, the optimal management is permanent interruption of the IVC.
- Necessary intraoperative care is required to preserve the collateral lumbar venous drainage, since these vessels provide a “release valve” for the impaired caval blood flow.
- Options for permanent interruption of the IVC include serrated vena cava clips (e.g., Adams-DeWeese clip, Moretz clip), cross stapling with a vascular GIA stapler (Covidien Ltd., Mansfield, MA), suture plication, and suture ligation.
- Perioperative complications
- Air embolism
- Potentially lethal
- Risk of air embolism can be significantly reduced by releasing the caudal IVC clamp first and allowing air and some blood (5 to 10 mL) to escape from the IVC repair site prior to removing the cranial clamp.
- Acute PE
- Tumor and bland thrombus can embolize during and after surgery. Minimizing intraoperative manipulation of the kidney and IVC before vascular control helps reduce the likelihood of acute thrombotic pulmonary embolism.
- If respiratory distress is encountered during surgery, strong consideration should be given to prompt thoracotomy, pulmonary arteriotomy, and extraction of the thrombus.
- Massive hemorrhage
- Major bleeding can occur during and after the surgery. If uncontrolled major bleeding occurs in a patient who is not on bypass, the surgeon should consider clamping the aorta above the celiac trunk or initiating deep hypothermic CPB
- Hepatic dysfunction
- Temporary hepatic dysfunction, characterized by elevated transaminases and alkaline phosphatase, is common in patients with levels III and IV thrombi that require suprahepatic IVC clamping and/or bypass.
- Liver enzymes typically peak 2 to 3 days postoperatively and slowly resolve thereafter.
- Organ ischemia
- Cardiac ischemia is most common in patients undergoing suprahepatic IVC clamping without bypass.
- Air embolism
Questions[edit | edit source]
- What are the potential benefit of renal artery embolization prior to nephrectomy?
- What are the indications for an adrenalectomy during radical nephrectomy?
- What are the indications for regional lymphadenectomy at the time of radical nephrectomy?
- When is a patch cavoplasty required during surgery for RCC with IVC thrombus?
- Patency of which artery is necessary for safe ligation of the inferior mesenteric artery?
- Describe the staging of IVC thrombi
- What is a potential consequence of ligating the superior mesenteric vein?
Answers[edit | edit source]
- What are the potential benefit of renal artery embolization prior to nephrectomy?
- Shrinkage of an arterialized tumor thrombus to ease surgical removal
- Reduced blood loss
- Facilitation of dissection as a result of tissue plane edema
- Modulation of immune response
- Ability to ligate the renal vein before the renal artery
- What are the indications for an adrenalectomy during radical nephrectomy?
- Adrenal mass on imaging
- Tumor thrombus
- Lymphadenopathy and regional metastasis
- Extrarenal tumor extension
- Large tumor size (>10 cm)
- Advanced stage (T3)
- Large upper pole tumors (>7cm) when the surgical plane between the kidney and adrenal gland may be compromised
- Diffuse involvement by tumor
- What are the indications for regional lymphadenectomy at the time of radical nephrectomy?
- Enlarged lymph nodes on imaging
- Cytoreductive surgery for metastatic disease
- Tumor size > than 10 cm
- Nuclear grade 3 or 4
- Sarcomatoid component
- Presence of tumor necrosis on imaging
- Extrarenal tumor extension
- Tumor thrombus
- Direct tumoral invasion of adjacent organs
- When is a patch cavoplasty required during surgery for RCC with IVC thrombus?
- If the IVC lumen is expected to be < 50% of its original size
- Patency of which artery is necessary for safe ligation of the inferior mesenteric artery?
- Marginal artery of the colon
- Describe the staging of IVC thrombi
- Level 0: no thrombus
- Level I: within 2cm of renal vein ostium
- Level II: below hepatic veins
- Level III: between hepatic veins and diaphragm
- Level IV: above diaphragm
- What is a potential consequence of ligating the superior mesenteric vein?
- Abdominal compartment syndrome; the abdomen should not be closed if the superior mesenteric vein is ligation
References[edit | edit source]
- Wein AJ, Kavoussi LR, Partin AW, Peters CA (eds): CAMPBELL-WALSH UROLOGY, ed 11. Philadelphia, Elsevier, 2015, chap 60
- Smith, Joseph A., et al. Hinman's Atlas of Urologic Surgery E-Book. Elsevier Health Sciences, 2016.